
Bone and Soft Tissue Pathology — MCQs

On this page
Which of the following bone tumors histologically resembles osteoblasts?
Which malignancy is characterized by large intracytoplasmic glycogen storage?
What are the characteristic microscopic features of Osteogenic sarcoma?
What is the most common malignant neoplasm of salivary gland origin that affects bones?
A 50-year-old woman presents with a painless soft tissue mass in her right thigh. Upon surgical excision, the surgeon notices that the tumor is adherent to the surrounding tissues. Histologic analysis reveals a neoplasm composed of pleomorphic clear cells, with vacuolated cytoplasm. The nucleus of many cells is indented by the cytoplasmic vacuoles, which are stained by histochemical methods for lipids. Which of the following is the most likely diagnosis?
Decreased mineralization of the epiphyseal plate in a growing child is seen in which condition?
A 25-year-old male patient presents with a bony expansile swelling of the right body of the mandible and mild paresthesia of the right inferior dental nerve. OPG shows a multilocular radiolucency without root resorption. What is odontogenic keratocyst noted for?
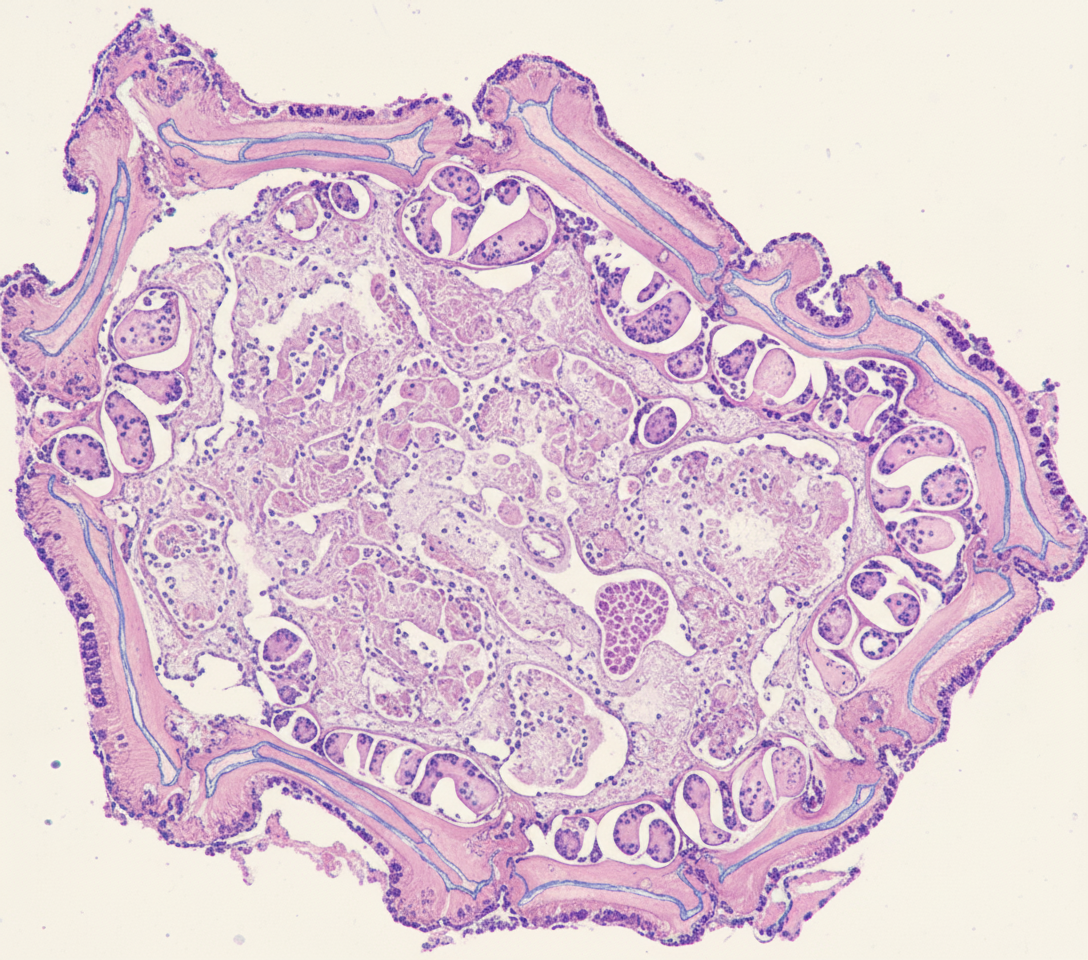
Histology of a biopsy from a long bone is shown below. Which of the following is the likely diagnosis?
Which tumor can occur following exposure to radiation?
Osteosarcoma originates from which type of cells?
Practice by Chapter
Bone Development and Growth
Practice Questions
Fracture Healing
Practice Questions
Osteomyelitis and Infectious Diseases
Practice Questions
Metabolic Bone Diseases
Practice Questions
Bone Tumors and Tumor-like Lesions
Practice Questions
Joints and Rheumatologic Diseases
Practice Questions
Soft Tissue Tumors
Practice Questions
Muscular Dystrophies and Myopathies
Practice Questions
Diseases of Tendons and Fascia
Practice Questions
Pathology of Orthopedic Implants
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app