
Bone and Soft Tissue Pathology — MCQs

On this page
In Duchenne muscular dystrophy, the defect is in the gene producing which protein?
A 47-year-old man presents with a 4-month history of dull, constant pain in the midsection of the right thigh. Physical examination reveals pain on palpation of the anterior right thigh, exacerbated by movement, and a larger circumference of the right thigh compared to the left. Radiography shows no fracture but an ill-defined soft-tissue mass anterior to the femur. MRI reveals a 10x8x7 cm solid mass deep to the quadriceps, without femur involvement. Karyotypic analysis of tumor cells shows t(12;16)(q13;p11) with amplification of the MDM2 gene. What is the most likely diagnosis?
In Duchenne's muscular dystrophy, what is the state of the calf muscle?
Calcification of the intervertebral disc is a feature of which condition?
Which of the following bone diseases characteristically exhibits a single lesion in a single bone?
Which of the following is TRUE about desmoid tumors?
What is the most common histological type of rhabdomyosarcoma?
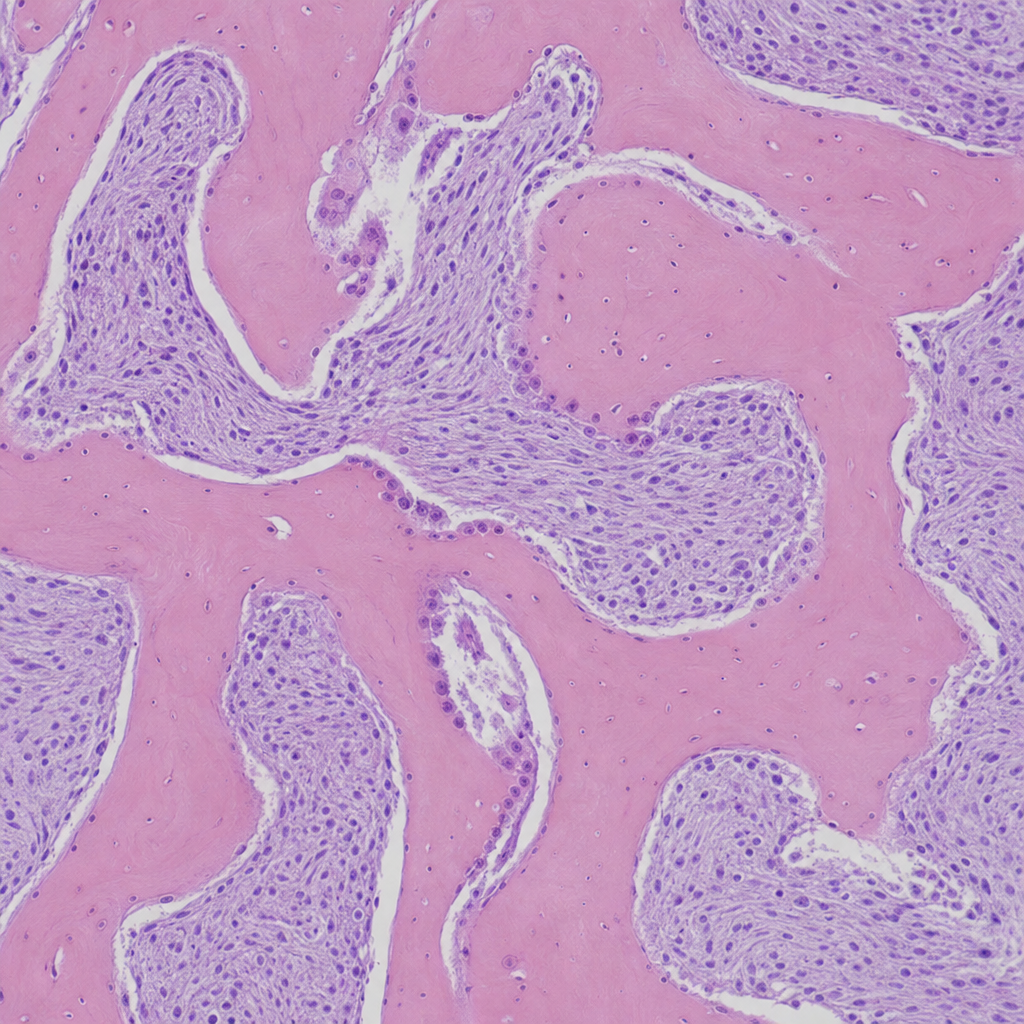
Histology from a bone biopsy of the proximal femur is shown for a 50-year-old patient presenting with bone pain. What is your diagnosis?
All of the following are malignant tumors except?
An African-American patient shows a radiolucent area surrounding the apices of mandibular anterior teeth which are vital. What is the most probable diagnosis?
Practice by Chapter
Bone Development and Growth
Practice Questions
Fracture Healing
Practice Questions
Osteomyelitis and Infectious Diseases
Practice Questions
Metabolic Bone Diseases
Practice Questions
Bone Tumors and Tumor-like Lesions
Practice Questions
Joints and Rheumatologic Diseases
Practice Questions
Soft Tissue Tumors
Practice Questions
Muscular Dystrophies and Myopathies
Practice Questions
Diseases of Tendons and Fascia
Practice Questions
Pathology of Orthopedic Implants
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app