
Principles of Fracture Management — MCQs

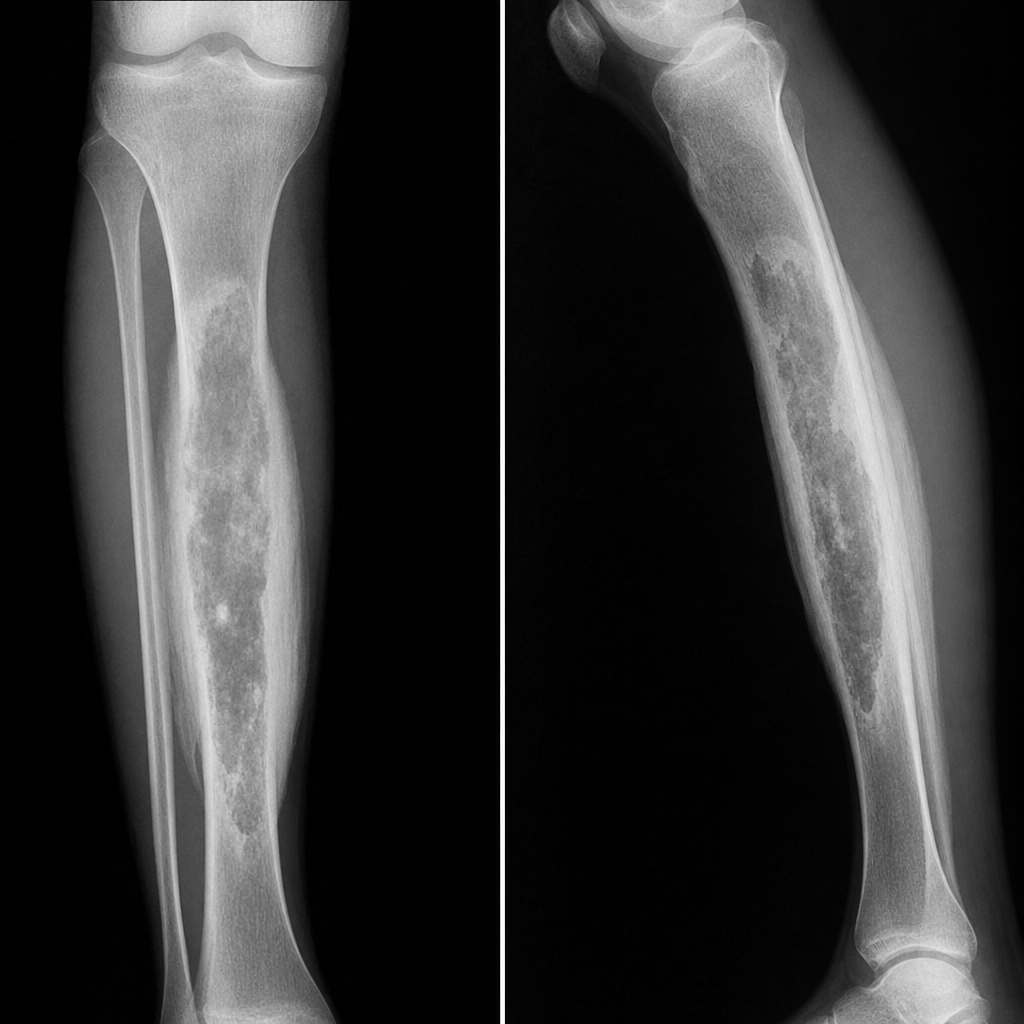
A patient has a history of RTA 2 years ago. He developed pain and swelling at the same site. What will be the diagnosis based on the provided X-ray features?
Management of Smith's fracture is
Treatment of choice in a 65-year-old female with impacted fracture of the neck of the humerus is:
First-line treatment for non-displaced scaphoid fracture
A patient fell off a bicycle and is now experiencing pain around the hip, shortening of the limb, and the hip is positioned in flexion, adduction, and internal rotation (IR). What is the most likely diagnosis?
Which nerve is commonly damaged in fracture of neck of fibula?
A patient came with history of fall and on examination there was tenderness between the extensor pollicis longus and brevis. The likely lesion is
Pilon fracture is
A patient fell off a bicycle and now complains of pain around the hip, with shortening of the affected limb. The hip is held in a position of flexion, adduction, and internal rotation. What is the most likely diagnosis?
All of the following are indications for open reduction and internal fixation (ORIF) of fractures EXCEPT:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app