
Shoulder Instability — MCQs

A patient received an electric shock and fell down. He cannot do external rotation of shoulder and cannot move arm. What is the diagnosis:-
Which of the following tests is used to test anterior instability of shoulder?
Tennis player can spontaneously reduce a shoulder dislocation. He can do it again and again himself. He is suffering from?
Which maneuver is used in the reduction of shoulder dislocation?
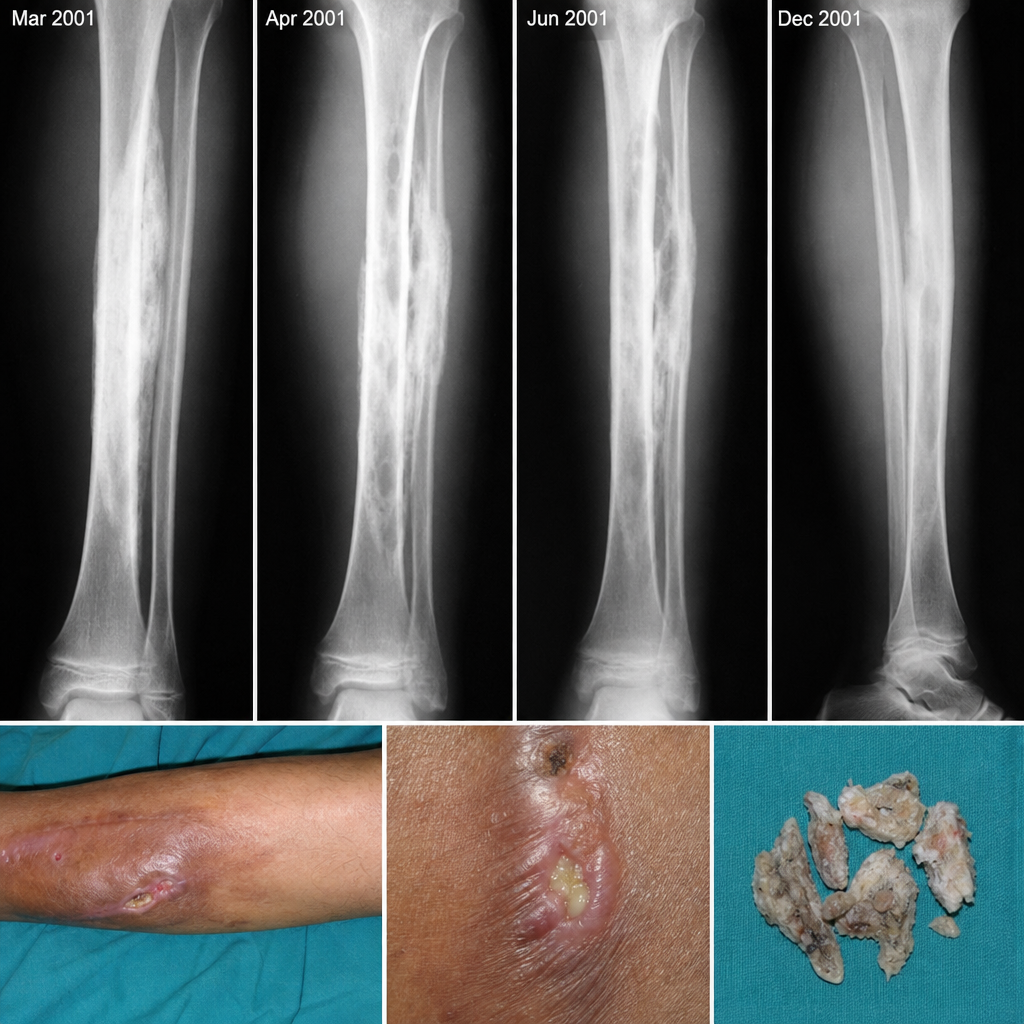
Which of the following statements is true regarding osteomyelitis?
A 25-year-old man presents to the emergency department after falling onto an outstretched hand while playing cricket. He has tenderness in the anatomical snuffbox and pain with axial loading of the thumb. What is the most likely diagnosis based on the X-ray findings?

In which condition is the Hamilton Ruler test sign positive?
Hill-Sachs lesion is seen in?
Patient had an injury to thumb causing thumb abduction. Which of the following can happen?
A 30-year-old male presents with pain and limited movement in his shoulder following a fall. X-ray reveals an anterior dislocation of the glenohumeral joint. Which of the following structures is most likely to be damaged in this injury?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app