
Sports Medicine — MCQs

On this page
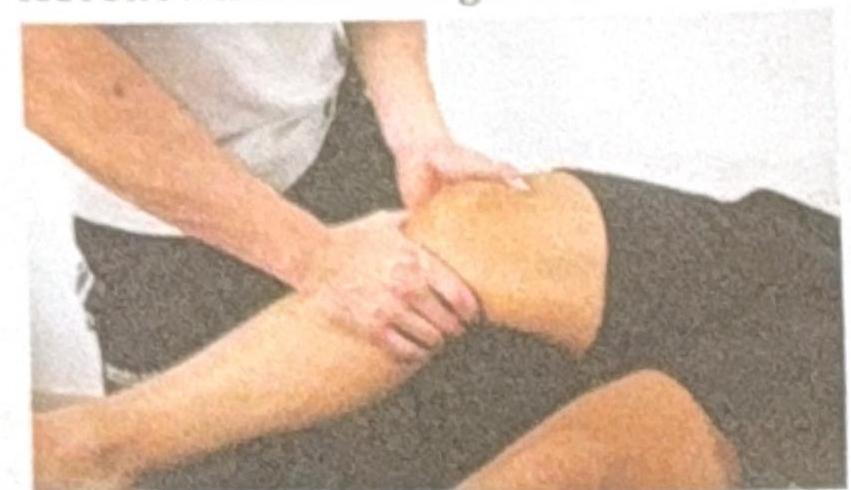
A football player experienced a twist in the ankle and knee. Clinically, no bone injury was appreciated. The examiner is performing the test shown in the image. Which test is this?
Football player with knee injury diagnosed as medial collateral ligament injury. Which structure is most commonly associated with this type of injury?
Tennis player can spontaneously reduce a shoulder dislocation. He can do it again and again himself. He is suffering from?
A 18-year-old boy was playing football when he suddenly twisted his knee and fell down. He got up after 10 minutes and resumed playing. The next day, he experienced knee swelling and difficulty moving it. What is the most probable cause?
In meniscus injury, 'Locking'-that is sudden inability to extend the knee fully is a feature of:
Which of the following tests is not done for anterior cruciate ligament injury?
Pivot shift test is positive with
Most common affected tendon in the Swimmer's shoulder?
Which of the following tests is used to test anterior instability of shoulder?
An athletic teenage girl complains of anterior knee pain on climbing stairs and on getting up after prolonged sitting. Which of the following is the most likely diagnosis?
Practice by Chapter
Sports Injuries: Epidemiology and Prevention
Practice Questions
Knee Ligament Injuries
Practice Questions
Meniscal Injuries
Practice Questions
Shoulder Instability
Practice Questions
Rotator Cuff Pathology
Practice Questions
Tendinopathies
Practice Questions
Muscle Strains and Contusions
Practice Questions
Ankle Sprains and Instability
Practice Questions
Overuse Injuries
Practice Questions
Return to Play Criteria
Practice Questions
Sports-Specific Conditioning
Practice Questions
Performance Enhancement
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app