
Sports Medicine — MCQs

On this page
Best initial treatment for acute calcific tendinitis of shoulder?
An 18-year-old athlete presents with acute knee pain and hemarthrosis after pivoting. The Lachman test is positive. Which ligament is most likely injured?
Which muscle is tested using the empty can test in shoulder injuries?
A 35-year-old athlete has persistent groin pain and a clicking sound during hip movements. MRI reveals labral tears and femoral acetabular impingement. What is the best intervention?
What is the most appropriate surgical management for a patient with a bucket-handle tear of the medial meniscus?
Which test is most commonly used to assess an anterior cruciate ligament (ACL) injury?
Which structures are typically involved in the 'unhappy triad' injury of the knee?
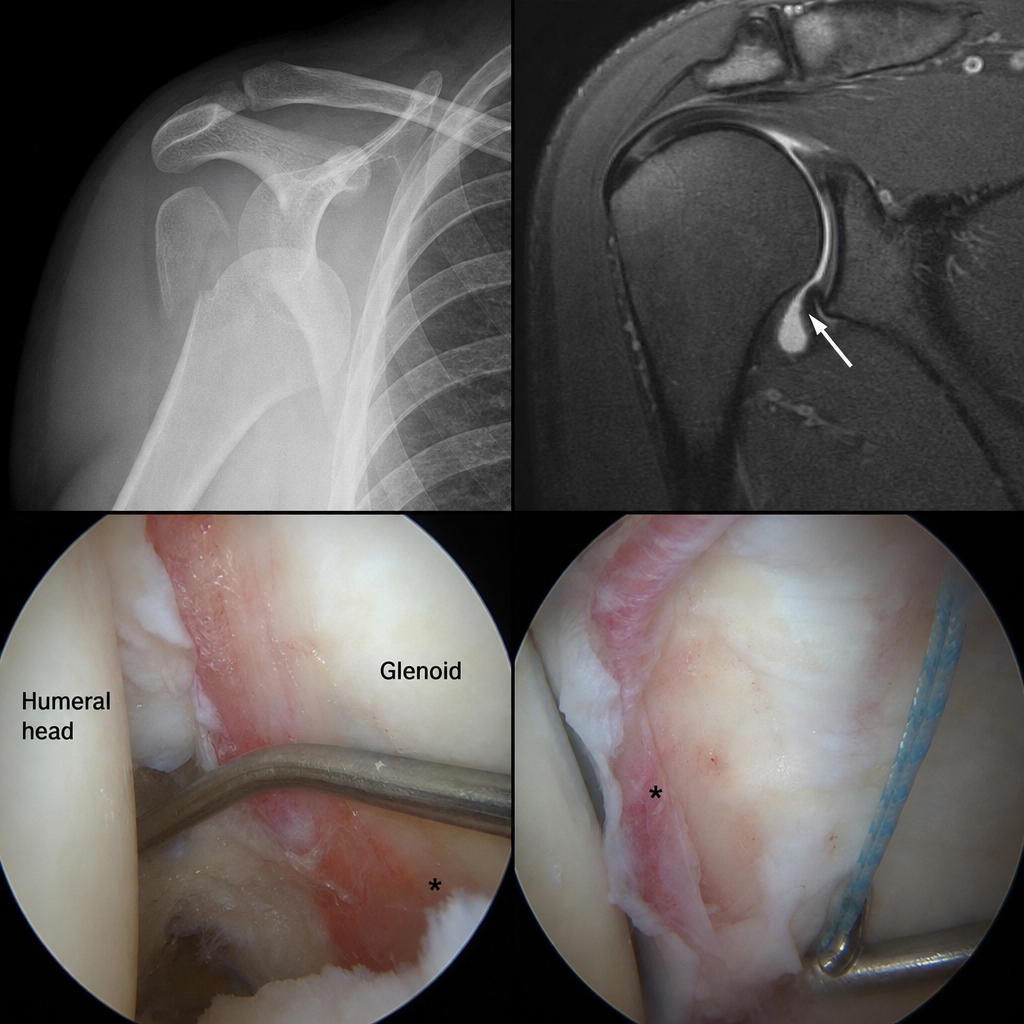
A 25-year-old athlete experiences recurrent anterior shoulder dislocations despite conservative management. Analyze the patient's condition using the provided image and suggest the most appropriate surgical intervention.
A young athlete complains of pain in the groin and weakness in the hip following a sports injury. An MRI shows a tear in which muscle that is commonly associated with groin injuries?
Which structure is commonly injured in a knee ligament tear?
Practice by Chapter
Sports Injuries: Epidemiology and Prevention
Practice Questions
Knee Ligament Injuries
Practice Questions
Meniscal Injuries
Practice Questions
Shoulder Instability
Practice Questions
Rotator Cuff Pathology
Practice Questions
Tendinopathies
Practice Questions
Muscle Strains and Contusions
Practice Questions
Ankle Sprains and Instability
Practice Questions
Overuse Injuries
Practice Questions
Return to Play Criteria
Practice Questions
Sports-Specific Conditioning
Practice Questions
Performance Enhancement
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app