
Pediatric Orthopaedics — MCQs

On this page
In treating a fractured clavicle in a 14-month-old child, what is the preferred management?
What is true regarding Jumper's Knee?
Which of the following associations between clinical angles and their corresponding conditions is incorrect?
A 10-year-old girl presents with a fall from a tree. Radiographic and physical examinations reveal Osgood-Schlatter disease. Which bony structure is chiefly affected in this condition?
Irregular thigh folds are seen in?
Which of the following is/are X-ray features of Legg-Calve-Perthes disease?
Which statement is NOT true regarding CTEV shoes?
A child presents with short stature and abnormalities of the hand and pelvis. What is your diagnosis?

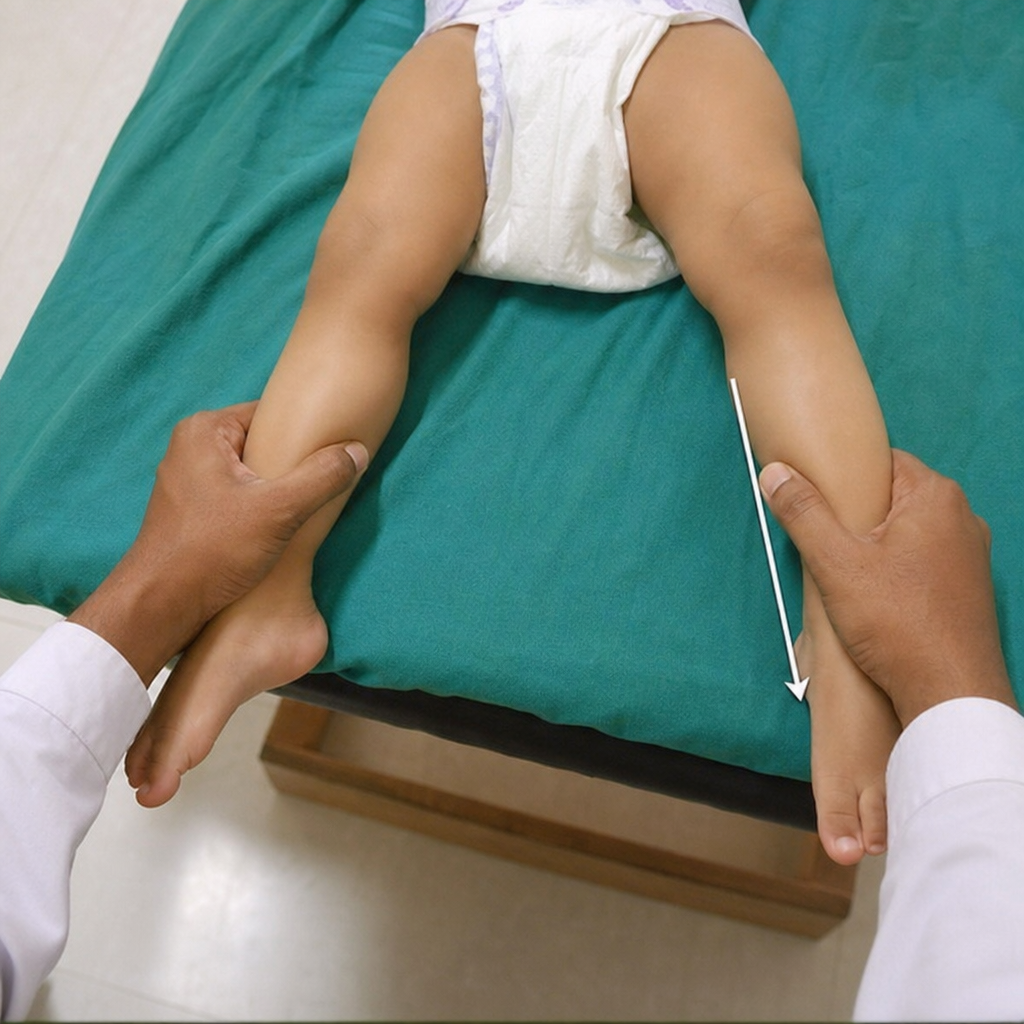
Which orthopedic test is being performed?
What is the most common fracture in childhood?
Practice by Chapter
Developmental Dysplasia of Hip
Practice Questions
Clubfoot
Practice Questions
Pediatric Fractures
Practice Questions
Growth Plate Injuries
Practice Questions
Legg-Calvé-Perthes Disease
Practice Questions
Slipped Capital Femoral Epiphysis
Practice Questions
Pediatric Spine Deformities
Practice Questions
Cerebral Palsy: Orthopaedic Aspects
Practice Questions
Neuromuscular Disorders in Children
Practice Questions
Pediatric Bone and Joint Infections
Practice Questions
Limb Length Discrepancies
Practice Questions
Orthopedic Manifestations of Genetic Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app