
Pediatric Orthopaedics — MCQs

On this page
What splint is used in CTEV after correction?
Von-Rosen's sign is positive in which of the following conditions?
What is the most common structural deformity associated with transient synovitis of the hip?
Which of the following is NOT a common fracture in children?
Madelung's deformity is characterized by an abnormality in which bone?
Which of the following movements is typically restricted in Perthes disease?
What is the primary pathology associated with Congenital Dislocation of the Hip (CDH)?
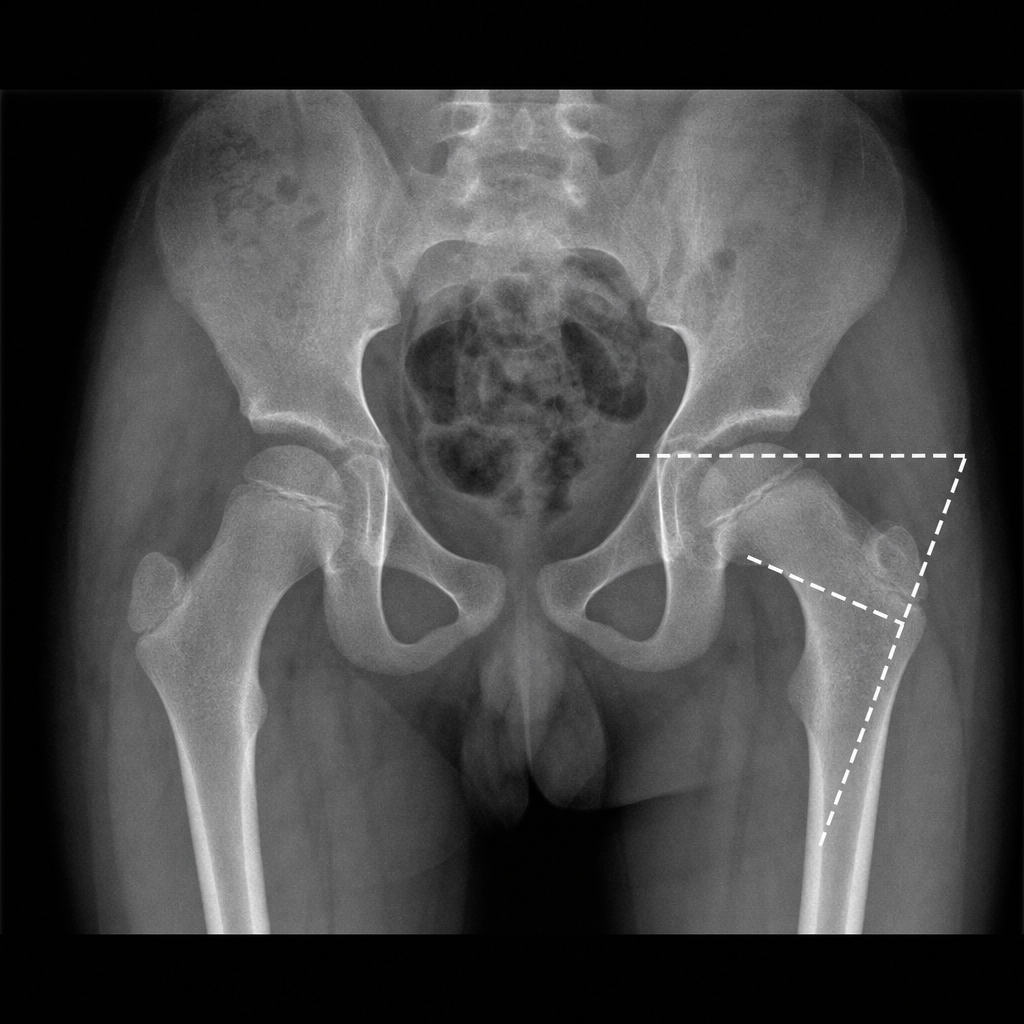
Fairbank triangle is seen in
Which of the following statements is true regarding supracondylar fractures of the humerus?
What is a Pulled Elbow?
Practice by Chapter
Developmental Dysplasia of Hip
Practice Questions
Clubfoot
Practice Questions
Pediatric Fractures
Practice Questions
Growth Plate Injuries
Practice Questions
Legg-Calvé-Perthes Disease
Practice Questions
Slipped Capital Femoral Epiphysis
Practice Questions
Pediatric Spine Deformities
Practice Questions
Cerebral Palsy: Orthopaedic Aspects
Practice Questions
Neuromuscular Disorders in Children
Practice Questions
Pediatric Bone and Joint Infections
Practice Questions
Limb Length Discrepancies
Practice Questions
Orthopedic Manifestations of Genetic Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app