
Pediatric Orthopaedics — MCQs

On this page
A 4-year-old child presents with fever and a mass in the thigh. An X-ray shows periosteal reaction and bone destruction. What is the next best step in diagnosis?
What is the most common type of fracture in children?
In pediatric patients, what is the most likely consequence of untreated developmental dysplasia of the hip?
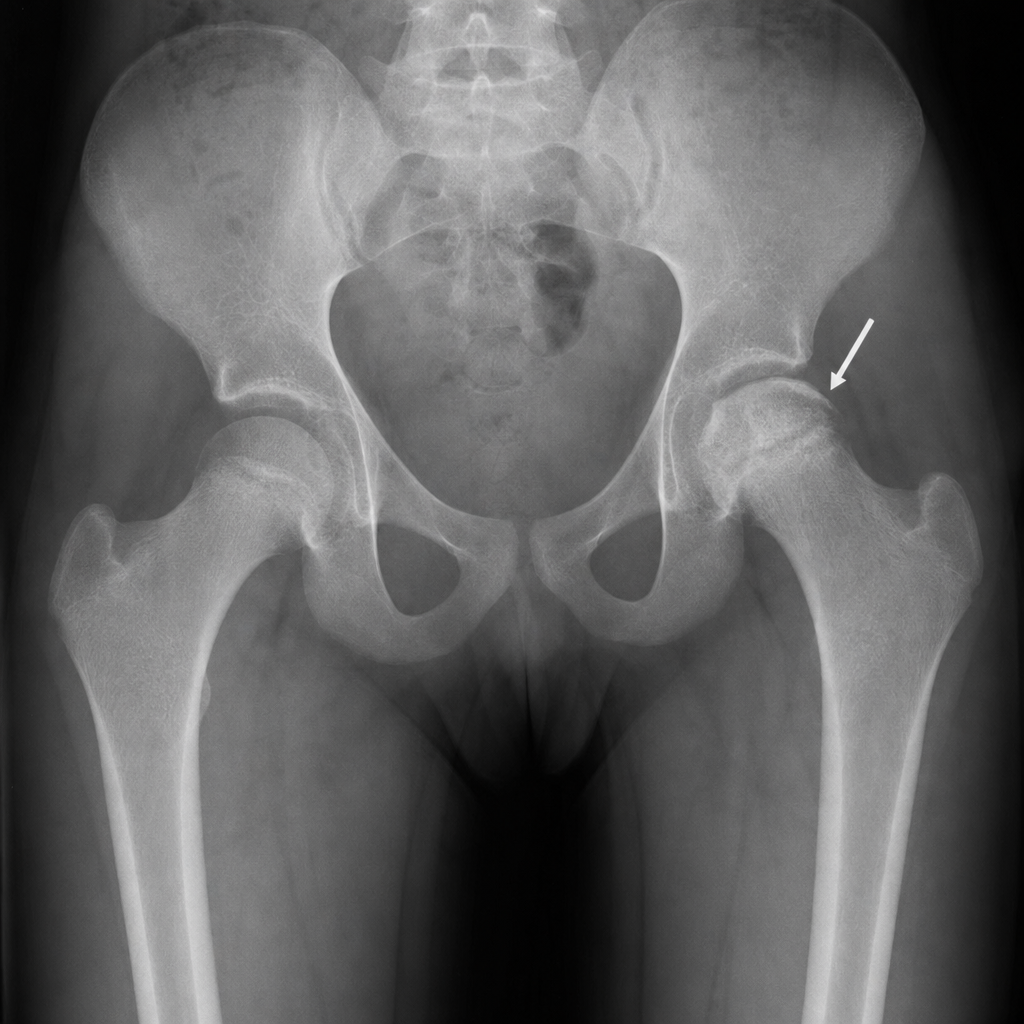
In a 12-year-old with a painless limp and limited hip abduction, an X-ray shows a crescent sign on the femoral head. What is the most likely diagnosis?
Which of the following statements about manipulation methods for correcting clubfoot (CTEV) is true?
Iliotibial band contracture in patients of poliomyelitis will lead to
Which deformity is the last to be corrected by Ponseti's method for CTEV?
Which of the following features are characteristic of Sprengel's deformity?
Which of the following statements about the tests for hip instability in neonates is not true?
All of the following are true regarding fracture of lateral condyle of humerus except:
Practice by Chapter
Developmental Dysplasia of Hip
Practice Questions
Clubfoot
Practice Questions
Pediatric Fractures
Practice Questions
Growth Plate Injuries
Practice Questions
Legg-Calvé-Perthes Disease
Practice Questions
Slipped Capital Femoral Epiphysis
Practice Questions
Pediatric Spine Deformities
Practice Questions
Cerebral Palsy: Orthopaedic Aspects
Practice Questions
Neuromuscular Disorders in Children
Practice Questions
Pediatric Bone and Joint Infections
Practice Questions
Limb Length Discrepancies
Practice Questions
Orthopedic Manifestations of Genetic Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app