
Pediatric Orthopaedics — MCQs

On this page
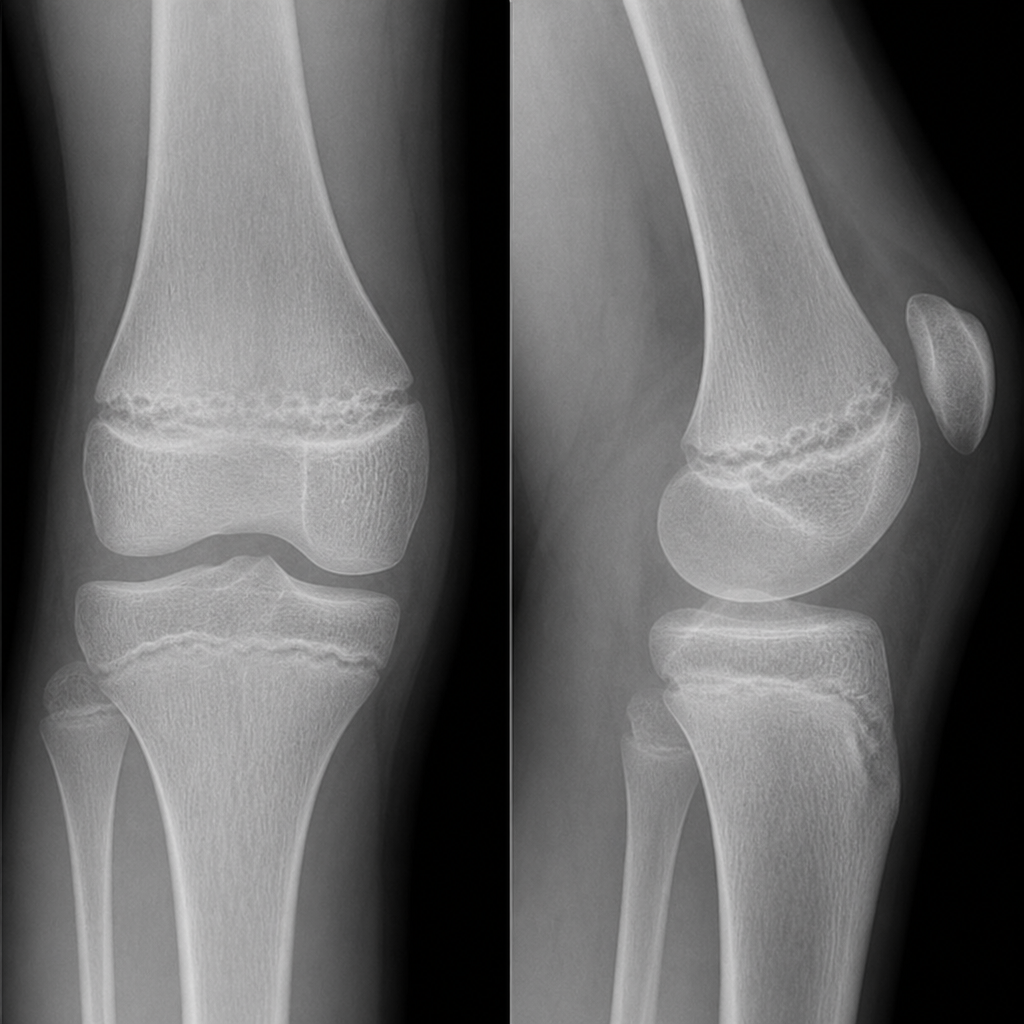
A 14-year-old presents with knee pain, limping, and progressive valgus deformity. X-ray shows a focal osseous bridge across the distal femoral physis with partial growth arrest. What is the diagnosis?
Which of the following best indicates poor prognosis in Developmental Dysplasia of Hip?
Fish tail deformity on X-ray in children is most commonly associated with fractures of?
Which Salter-Harris fracture type involves a metaphyseal fragment?
A teenage boy presents with a painful lump below his knee. Which condition involving inflammation of the tibial tuberosity is most likely?
A 12-year-old boy presents with a limp and knee pain. X-rays reveal a slipped capital femoral epiphysis. What is the most appropriate initial management?
A 9-year-old with recent onset of limping, no history of trauma, and intermittent knee pain. Physical examination shows decreased hip range of motion and a normal knee exam. X-ray reveals a flattened femoral head. What is the next step in evaluation and management?
In a pediatric patient with a displaced supracondylar fracture of the humerus, what is the most appropriate treatment?
A 6-year-old child presents with a limp and limited hip abduction. An X-ray reveals flattening of the femoral head. What is the most likely diagnosis?

What is the most common cause of scoliosis in pediatric patients?
Practice by Chapter
Developmental Dysplasia of Hip
Practice Questions
Clubfoot
Practice Questions
Pediatric Fractures
Practice Questions
Growth Plate Injuries
Practice Questions
Legg-Calvé-Perthes Disease
Practice Questions
Slipped Capital Femoral Epiphysis
Practice Questions
Pediatric Spine Deformities
Practice Questions
Cerebral Palsy: Orthopaedic Aspects
Practice Questions
Neuromuscular Disorders in Children
Practice Questions
Pediatric Bone and Joint Infections
Practice Questions
Limb Length Discrepancies
Practice Questions
Orthopedic Manifestations of Genetic Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app