
Pediatric Orthopaedics — MCQs

On this page
An adolescent presents with activity-related anterior knee pain and tenderness over the tibial tubercle. Identify the condition shown in the given X-ray:

The image shows a displaced pediatric supracondylar humeral fracture. Which classification system and stage best describes this fracture?

Combination of appearance in CTEV
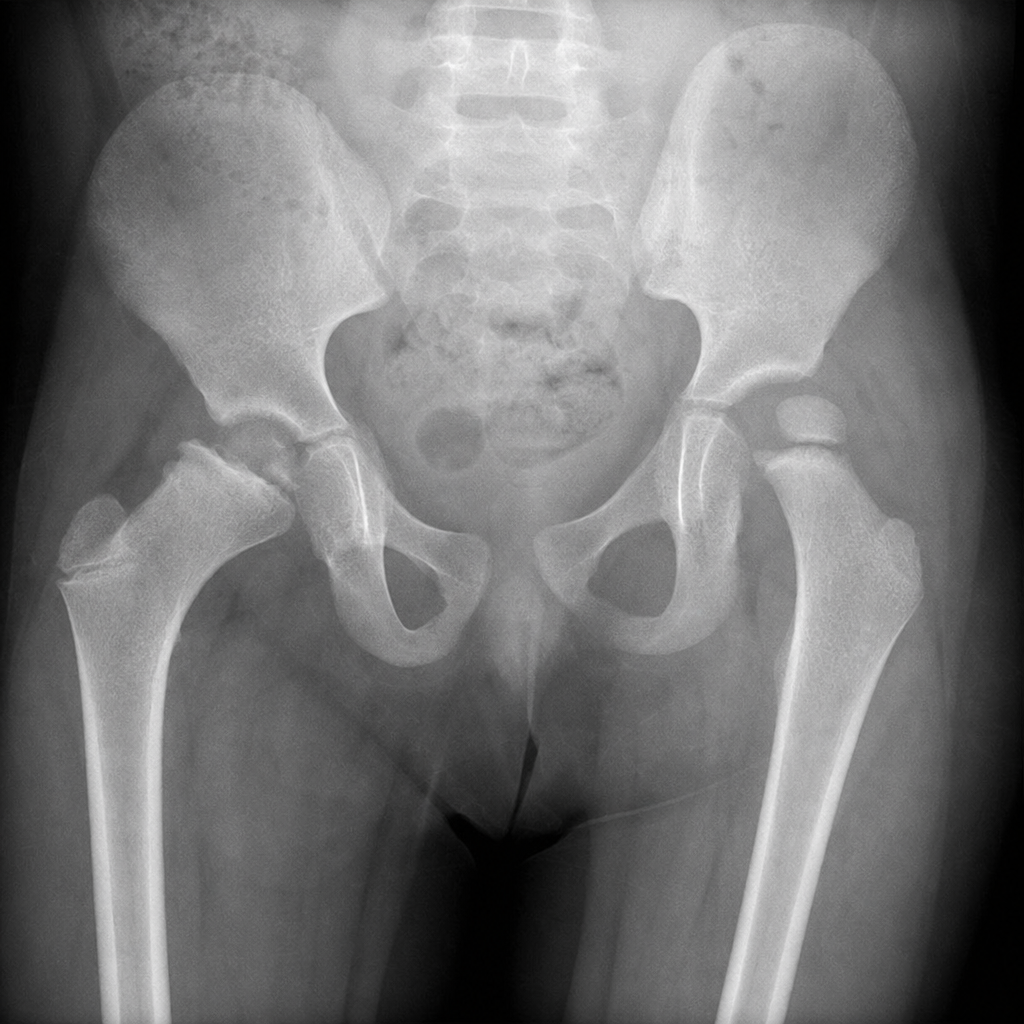
A 13-year-old Hispanic boy is brought to the physician by his mother because of left groin pain for 1 month. The pain radiates to his left knee and is aggravated on walking. He fell during soccer practice 5 weeks ago but did not see a doctor about it and does not recall any immediate and persistent pain after the event. He has hypothyroidism. His only medication is levothyroxine. His immunizations are up-to-date. He appears uncomfortable. He is at the 50th percentile for height and at the 95th percentile for weight. His temperature is 37.1°C (98.9°F), pulse is 77/min, respirations are 14/min, and blood pressure is 100/70 mm Hg. The patient has a left-sided, antalgic gait. The left lower extremity is externally rotated. The left hip is tender to palpation and internal rotation is limited by pain. Laboratory studies show: Hemoglobin 13.1 g/dL Leukocyte count 9,100/mm3 Platelet count 250,000/mm3 Serum TSH 3.6 μU/mL Which of the following is the most likely diagnosis?
Blount Disease is involvement of
A 6-year-old child is suspected with supracondylar fracture of right hand, complaining of pain and swelling. X-ray of right elbow was not significant. What is the next best step in this case?
A child presents with a limp and limb shortening. The X-ray is shown below. What is the diagnosis?
Most common site of osteomyelitis in children
Charlie Chaplin gait is seen in?
Omovertebral bone is associated with?
Practice by Chapter
Developmental Dysplasia of Hip
Practice Questions
Clubfoot
Practice Questions
Pediatric Fractures
Practice Questions
Growth Plate Injuries
Practice Questions
Legg-Calvé-Perthes Disease
Practice Questions
Slipped Capital Femoral Epiphysis
Practice Questions
Pediatric Spine Deformities
Practice Questions
Cerebral Palsy: Orthopaedic Aspects
Practice Questions
Neuromuscular Disorders in Children
Practice Questions
Pediatric Bone and Joint Infections
Practice Questions
Limb Length Discrepancies
Practice Questions
Orthopedic Manifestations of Genetic Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app