
Pediatric Orthopaedics — MCQs

On this page
The following gait is called as hand knee gait. Normally to transmit the weight of limb during midstance, the knee is locked by quadriceps contraction. If it is weak, locking is hampered and buckling at knees will occur. Hence to stabilise the knee for weight bearing, patient places his hand in front of knee and lower thigh region. This gait pattern is typically seen in which condition?

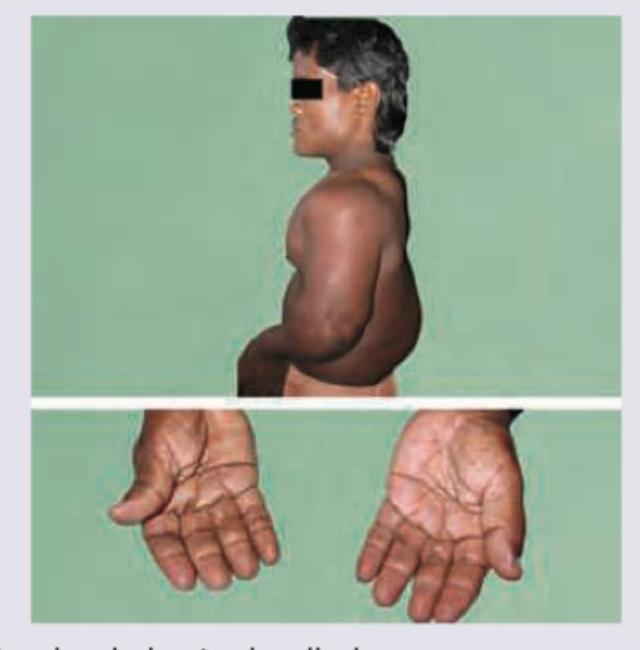
Which is incorrect about the patient shown in the image? (Recent NEET Pattern 2016-17)
A patient presents with the gait abnormality shown in the image. On examination, there is loss of pain and temperature sensation over the dorsum of the foot in a glove-and-stocking distribution, and the common peroneal nerve is palpably thickened at the fibular head. The following gait abnormality is seen in:

The following X-ray pelvis of a child shows:

The priority in management of supracondylar fracture of humerus in a child is:
The prognosis in reduced or unreduced fractures involving epiphyseal plate is very poor if the fracture line:
Kohler's disease is avascular necrosis of :
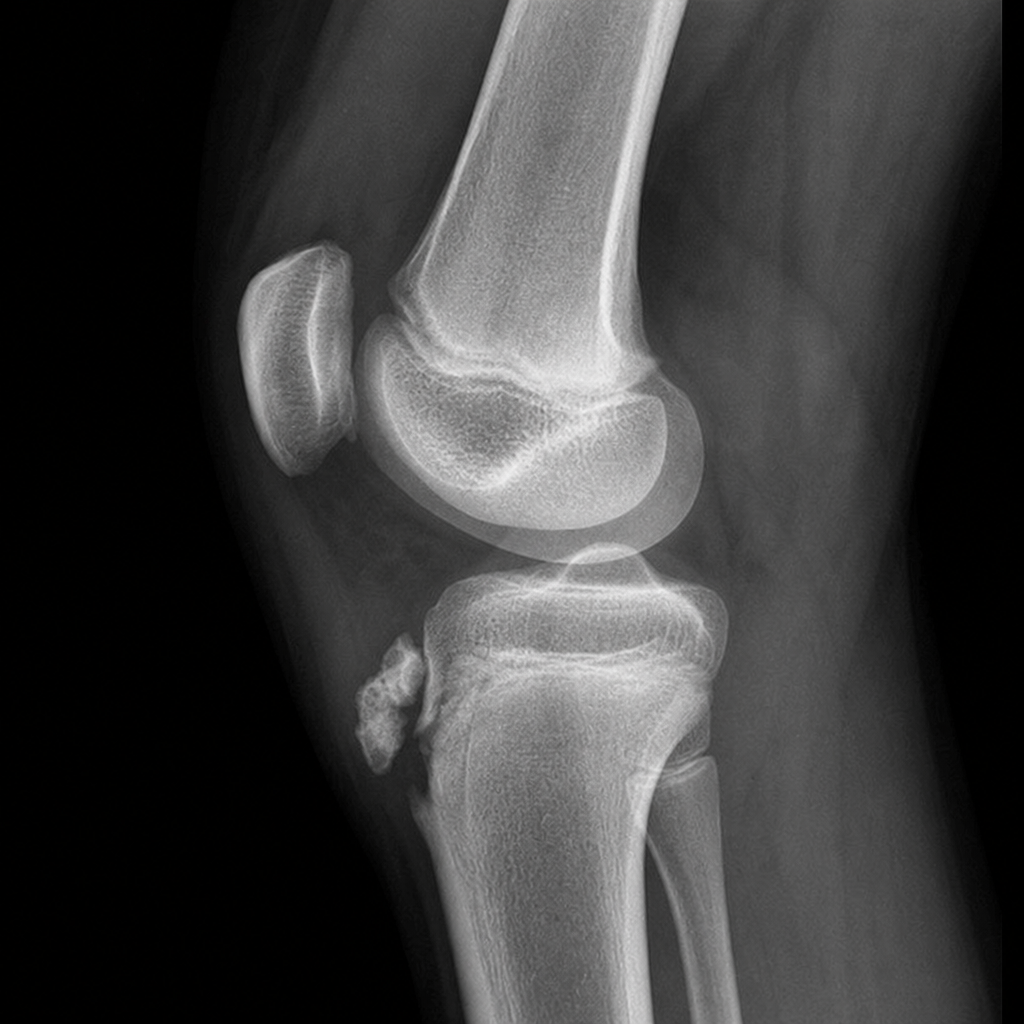
A 13-year-old male presents with gradual-onset pain, swelling, and tenderness at the tibial tuberosity, worsening with physical activity. Identify the condition shown in the given X-ray: 
Fracture at which site affects the longitudinal growth of a bone?
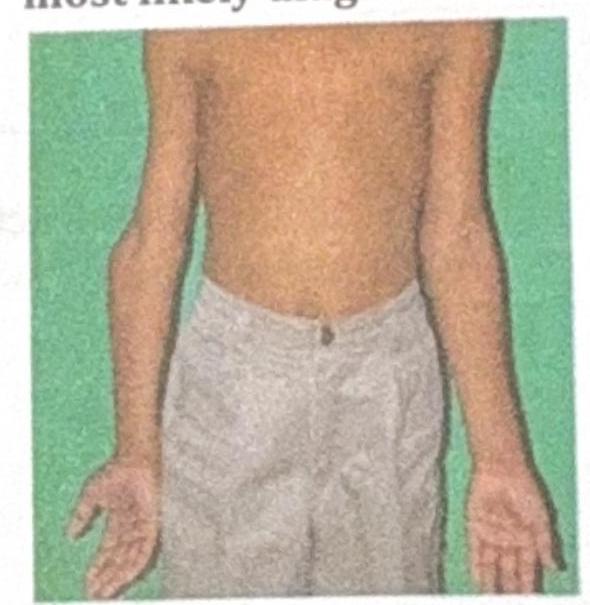
A 10-year-old boy presents with the physical findings shown in the image, characterized by inward angulation of the elbows. What is the most likely diagnosis?
Practice by Chapter
Developmental Dysplasia of Hip
Practice Questions
Clubfoot
Practice Questions
Pediatric Fractures
Practice Questions
Growth Plate Injuries
Practice Questions
Legg-Calvé-Perthes Disease
Practice Questions
Slipped Capital Femoral Epiphysis
Practice Questions
Pediatric Spine Deformities
Practice Questions
Cerebral Palsy: Orthopaedic Aspects
Practice Questions
Neuromuscular Disorders in Children
Practice Questions
Pediatric Bone and Joint Infections
Practice Questions
Limb Length Discrepancies
Practice Questions
Orthopedic Manifestations of Genetic Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app