
Pediatric Orthopaedics — MCQs

On this page
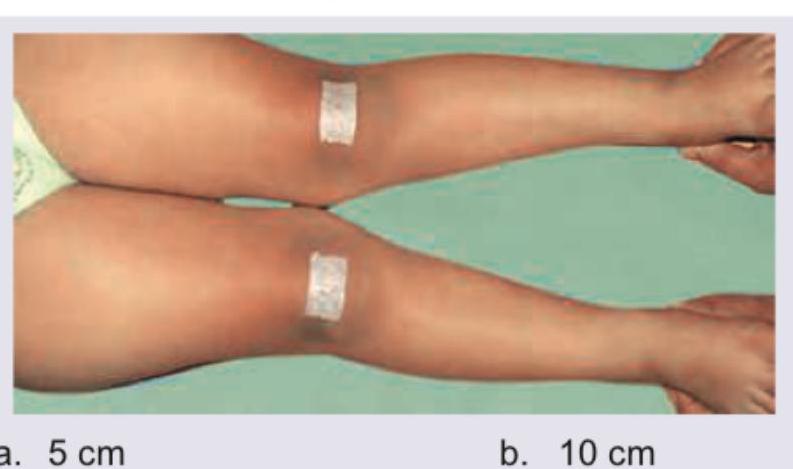
The clinical presentation of 9-year-old child is shown below. Work up for rickets showed normal serum calcium, phosphate and serum alkaline phosphatase. The deformity is persistent and progressive, with mechanical-axis deviation and symptoms, and the child has sufficient remaining growth. According to the traditionally cited examination threshold, surgery is considered if the intermalleolar distance exceeds \qquad .
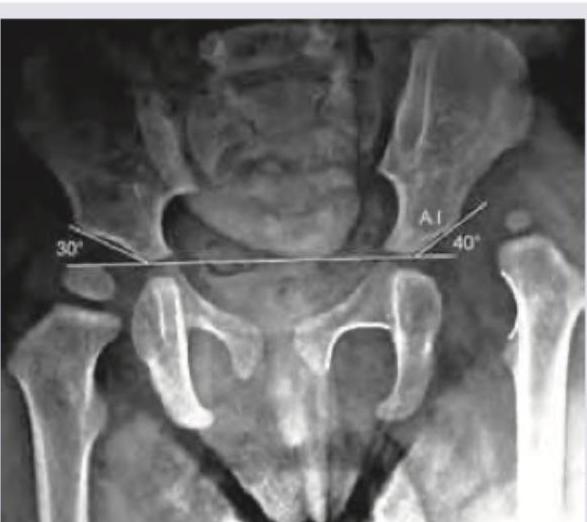
A 5-year-old child presents with limp and pain in left thigh. The mother remarks that her child was always very active and was always running and jumping around, but has restricted activity for last 3 months. What does the given X-ray bilateral hip joint show?

Comment on the diagnosis in the X-ray pelvis of a 2-year-old child as shown below:
All are true about the condition shown in the image except:
All are correct about the condition shown in the image except:

A 4-year-old boy fell on outstretched hand. X- Ray is shown below. Which blood vessel is most commonly affected?

Given is the X-ray of a 7-year-old child. Identify the deformity:

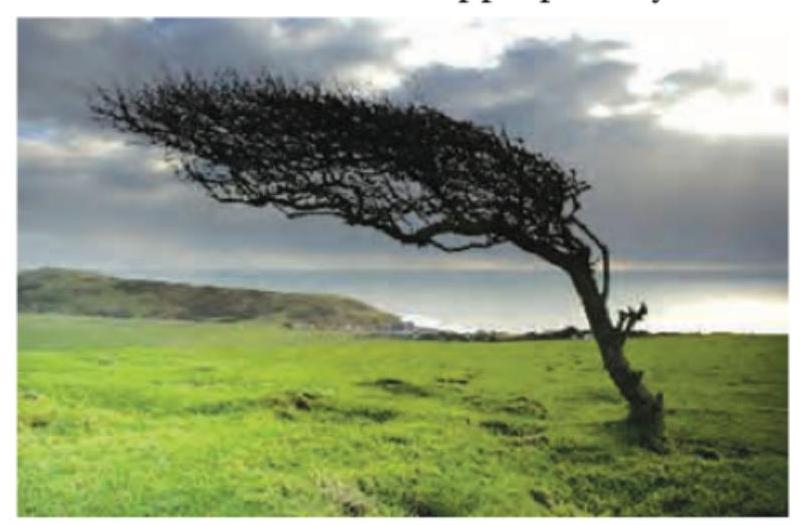
The image shows an analogy used to describe a specific orthopedic deformity. Which deformity is characterized by varus deformity in one lower limb combined with valgus deformity in the other lower limb?
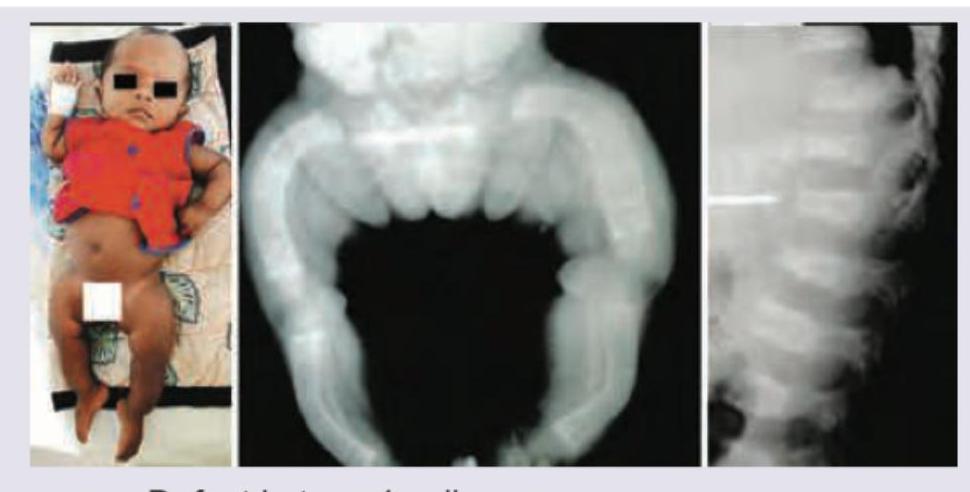
A 3-month-old infant with shortened bowed extremities, macrocephaly. X-ray of lower extremities and Lateral view spine was performed. All are true about classic COL1A1/COL1A2-related osteogenesis imperfecta except: (Recent NEET Pattern 2016-17)
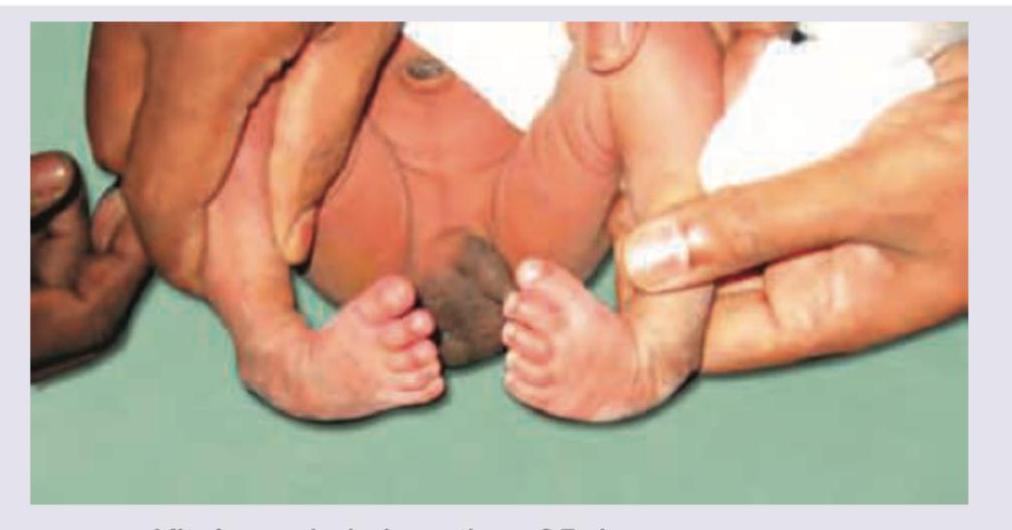
The image shows presence of:
Practice by Chapter
Developmental Dysplasia of Hip
Practice Questions
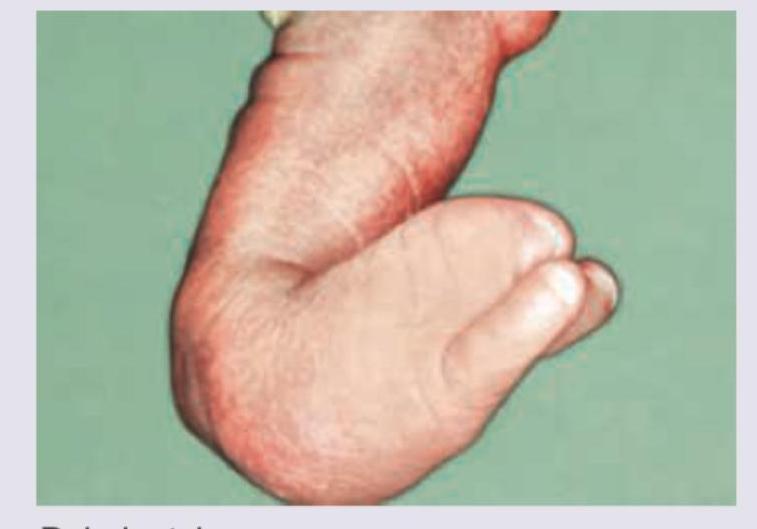
Clubfoot
Practice Questions
Pediatric Fractures
Practice Questions
Growth Plate Injuries
Practice Questions
Legg-Calvé-Perthes Disease
Practice Questions
Slipped Capital Femoral Epiphysis
Practice Questions
Pediatric Spine Deformities
Practice Questions
Cerebral Palsy: Orthopaedic Aspects
Practice Questions
Neuromuscular Disorders in Children
Practice Questions
Pediatric Bone and Joint Infections
Practice Questions
Limb Length Discrepancies
Practice Questions
Orthopedic Manifestations of Genetic Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app