
Pediatric Orthopaedics — MCQs

On this page
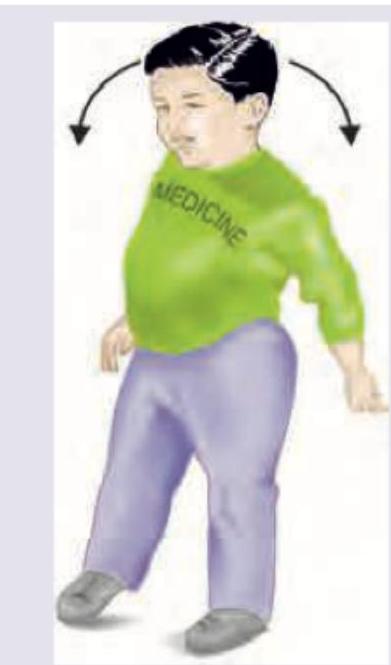
Image shown below depicts:

All are correct about the image shown except:

Incorrect about the image is:

All are true about the test being performed except:

The following gait is due to:
Comment on the diagnosis on the case presentation shown:

A 10-year-old obese boy has pain in the left groin after slipping during a basketball match 4 weeks back. On examination he has limitation of internal rotation. What does the given X-ray bilateral hip joint show?

What does X-ray pelvis show?

What does the image given below show?

A 3-year-old obese child presents with a leg deformity as shown. On work up, the plasma ascorbate levels are normal. Serum calcium, phosphate and serum alkaline phosphatase are normal. X-ray of bilateral knee joint is shown below. What is the diagnosis?

Practice by Chapter
Developmental Dysplasia of Hip
Practice Questions
Clubfoot
Practice Questions
Pediatric Fractures
Practice Questions
Growth Plate Injuries
Practice Questions
Legg-Calvé-Perthes Disease
Practice Questions
Slipped Capital Femoral Epiphysis
Practice Questions
Pediatric Spine Deformities
Practice Questions
Cerebral Palsy: Orthopaedic Aspects
Practice Questions
Neuromuscular Disorders in Children
Practice Questions
Pediatric Bone and Joint Infections
Practice Questions
Limb Length Discrepancies
Practice Questions
Orthopedic Manifestations of Genetic Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app