
Pediatric Orthopaedics — MCQs

On this page
What is true about Salter-Harris type IV epiphyseal injury?
A 6-year-old child sustained an elbow injury. Four years later, the child presents with tingling and numbness on the ulnar side of the fingers. What type of fracture is most likely associated with these symptoms?
Cubitus varus deformity in supracondylar fracture of humerus is usually due to which of the following?
What is meant by a 'pulled elbow'?
Ortolani's test is done for which condition?
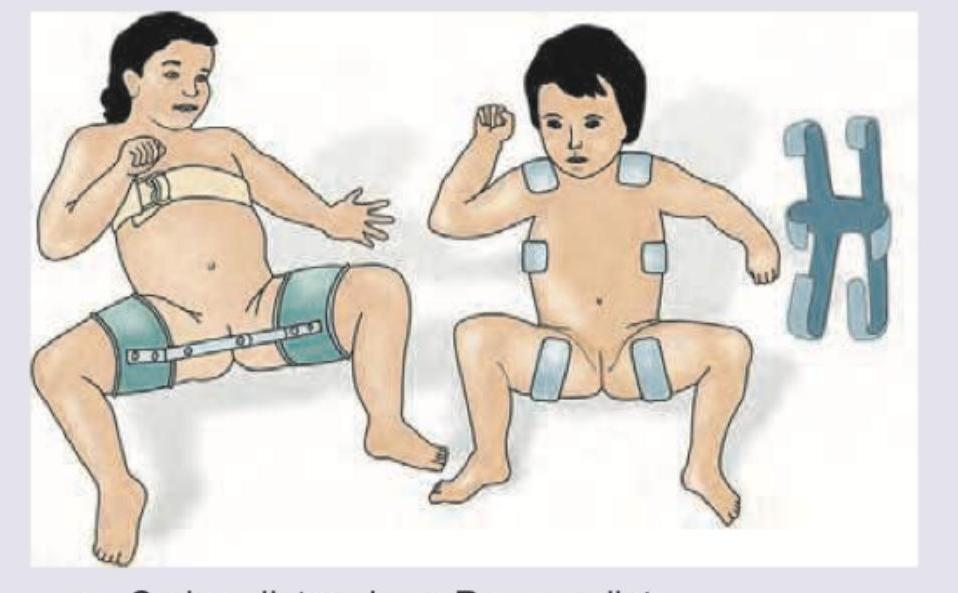
Which of the following splints is shown in the image?

Which is correct about the image shown below?
A 3-year-child fell from the roof and landed on his feet. What is the Salter and Harris grading of the fracture in distal tibia as shown below?

A 7-year-old child presents to the emergency department after a fall on an outstretched hand. The following X-ray of the elbow shows:

A 12-year-old boy while playing football falls over a goalpost and hurts his arm. X-ray forearm was performed. What is the most likely diagnosis?

Practice by Chapter
Developmental Dysplasia of Hip
Practice Questions
Clubfoot
Practice Questions
Pediatric Fractures
Practice Questions
Growth Plate Injuries
Practice Questions
Legg-Calvé-Perthes Disease
Practice Questions
Slipped Capital Femoral Epiphysis
Practice Questions
Pediatric Spine Deformities
Practice Questions
Cerebral Palsy: Orthopaedic Aspects
Practice Questions
Neuromuscular Disorders in Children
Practice Questions
Pediatric Bone and Joint Infections
Practice Questions
Limb Length Discrepancies
Practice Questions
Orthopedic Manifestations of Genetic Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app