
Pediatric Orthopaedics — MCQs

On this page
All of the following are true about a pulled elbow except?
The Kebab treatment is used for the treatment of which of the following conditions?
French osteotomy is used in the treatment of which condition?
Which statement is not true about Perthes disease?
What is the treatment for congenital coxa vara?
A 16-year-old boy presents with progressive knee pain that began soon after starting basketball season. Physical examination reveals a swollen and prominent tibial tubercle with associated tenderness. Radiographs of the area are unremarkable. What is the most likely diagnosis?
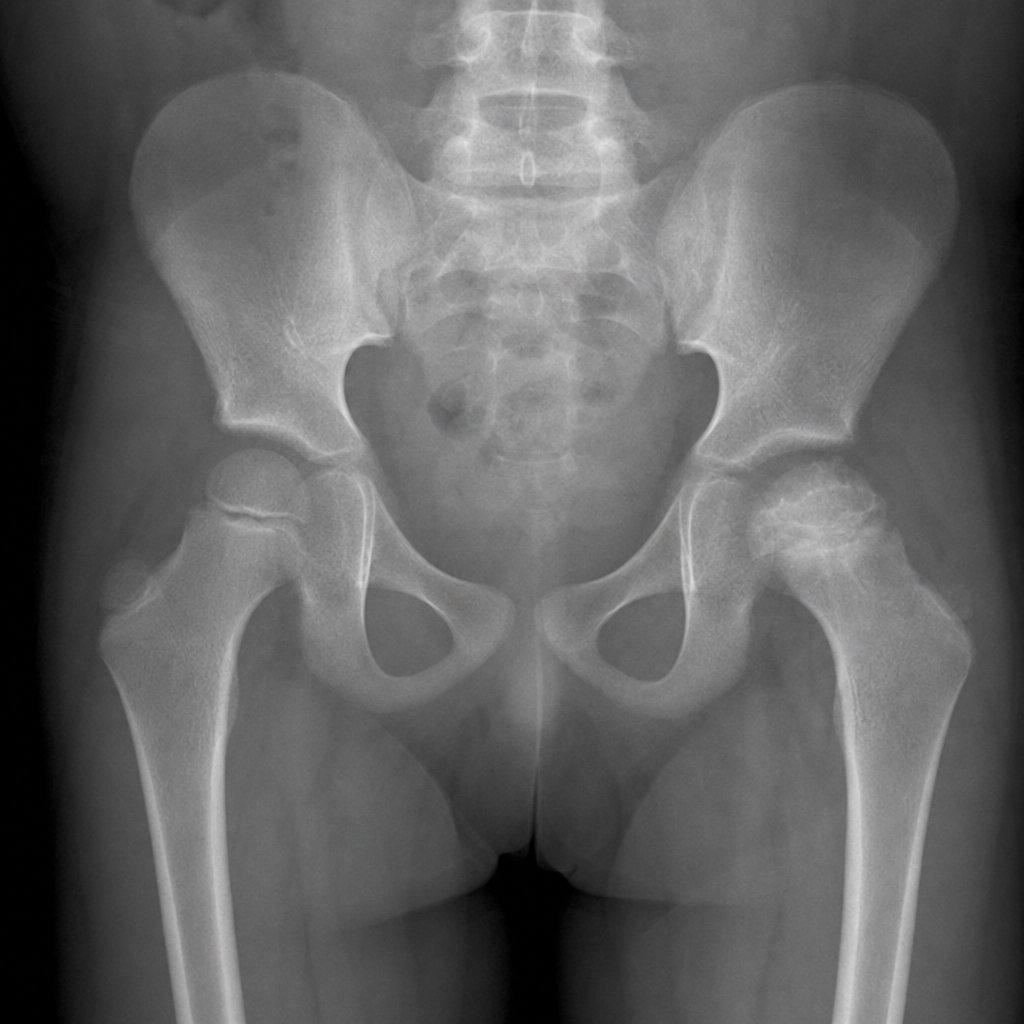
A 17-year-old presents with acute atraumatic hip pain, fever of 39.2°C, inability to bear weight, and severe pain with passive hip movement. The leukocyte count, ESR, and CRP are elevated. The AP pelvis radiograph shown reveals no acute osseous abnormality. Which is the most appropriate next step to confirm the suspected diagnosis?
Which of the following statements regarding supracondylar fracture of the humerus in children is true?
All of the following are associated with supracondylar fracture of humerus, except?
A 40-year-old patient presents with an inability to keep the arm in contact with the chest. When the arm is forcibly brought into contact with the chest, there is winging of the scapula. There is a history of repeated intramuscular injections into the deltoid muscle. What is the diagnosis?
Practice by Chapter
Developmental Dysplasia of Hip
Practice Questions
Clubfoot
Practice Questions
Pediatric Fractures
Practice Questions
Growth Plate Injuries
Practice Questions
Legg-Calvé-Perthes Disease
Practice Questions
Slipped Capital Femoral Epiphysis
Practice Questions
Pediatric Spine Deformities
Practice Questions
Cerebral Palsy: Orthopaedic Aspects
Practice Questions
Neuromuscular Disorders in Children
Practice Questions
Pediatric Bone and Joint Infections
Practice Questions
Limb Length Discrepancies
Practice Questions
Orthopedic Manifestations of Genetic Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app