
Pediatric Orthopaedics — MCQs

On this page
What is the ideal age for performing a Posterior Malleolar Stress Test (PMSTR)?
What is the most common associated injury with a fracture of the medial epicondyle?
The Ortolani test is considered positive when the examiner hears which of the following?
A 16-year-old obese female presents with a history of bilateral hip pain of long duration and a painful, limping gait. Endocrinology tests show hypothyroidism. Which of the following investigations is of no use in the diagnosis of this condition?
Surgical excision is contraindicated in which of the following anatomical structures?
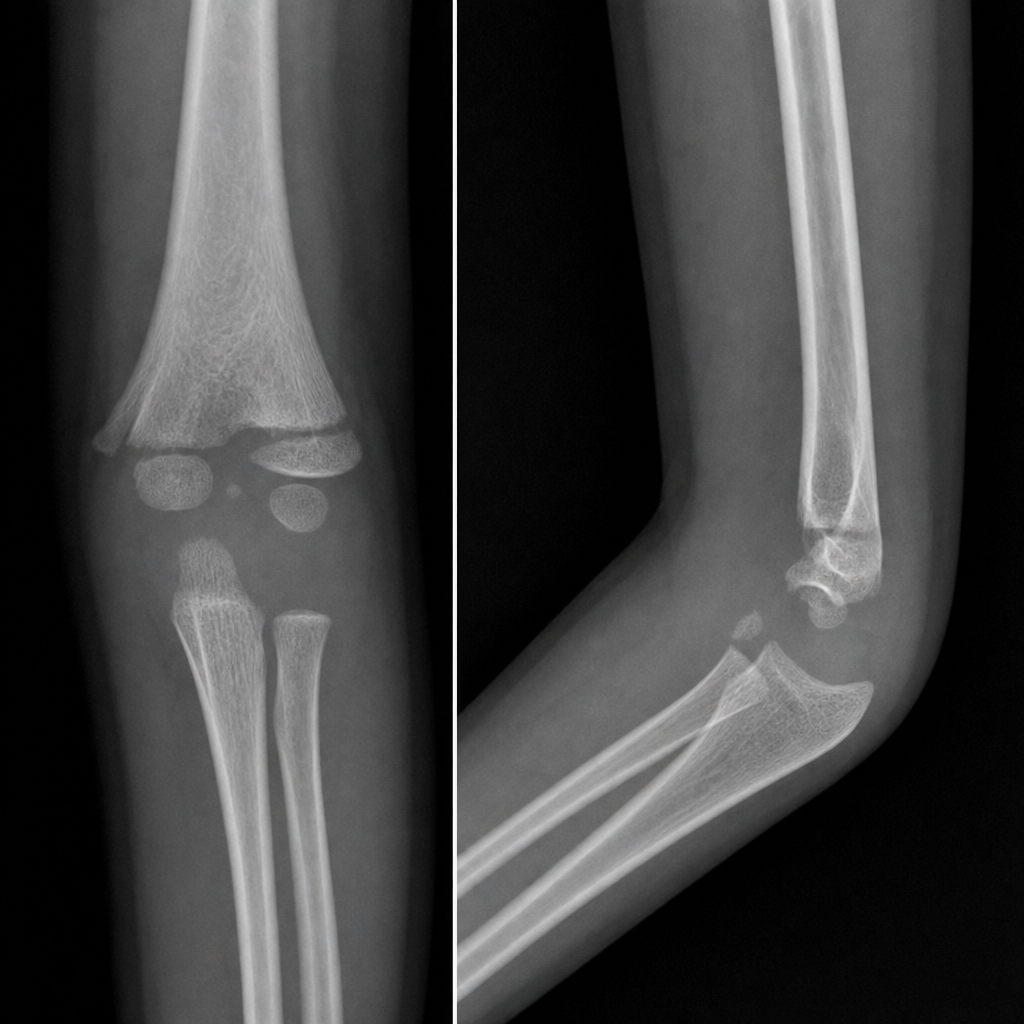
A 5-year-old child presents to your clinic. Which is the most likely fracture shown in the elbow radiographs?
Congenital talipes equinovarus (CTEV) is caused by all of the following except?
A child presents with hip pain. X-ray of the pelvis shows generalized osteopenia, thin cortices, gracile long bones, and proximal femoral deformity with evidence of healed fractures. What is the most likely clinical diagnosis?
Which of the following is a musculoskeletal abnormality associated with neurofibromatosis?
How is a pulled elbow treated?
Practice by Chapter
Developmental Dysplasia of Hip
Practice Questions
Clubfoot
Practice Questions
Pediatric Fractures
Practice Questions
Growth Plate Injuries
Practice Questions
Legg-Calvé-Perthes Disease
Practice Questions
Slipped Capital Femoral Epiphysis
Practice Questions
Pediatric Spine Deformities
Practice Questions
Cerebral Palsy: Orthopaedic Aspects
Practice Questions
Neuromuscular Disorders in Children
Practice Questions
Pediatric Bone and Joint Infections
Practice Questions
Limb Length Discrepancies
Practice Questions
Orthopedic Manifestations of Genetic Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app