
Pediatric Orthopaedics — MCQs

On this page
A 2-year-old child with a history of old knee injury now has varus deformity of the left knee. Deformity persists on flexion; blood report is normal. X-ray shows unilateral genu varum and angulated tibia. What is the diagnosis?
A child presents with a Gower sign. What does this finding indicate?
Epiphyseal enlargement is seen in which of the following conditions?
Slipped capital femoral epiphysis is seen most commonly in which age group?
A 4-year-old child sustained a fall on an outstretched hand. X-rays revealed a fracture line at the physis with a small metaphyseal fragment. There was no epiphyseal fracture. What type of injury, according to the Salter-Harris classification, is this?
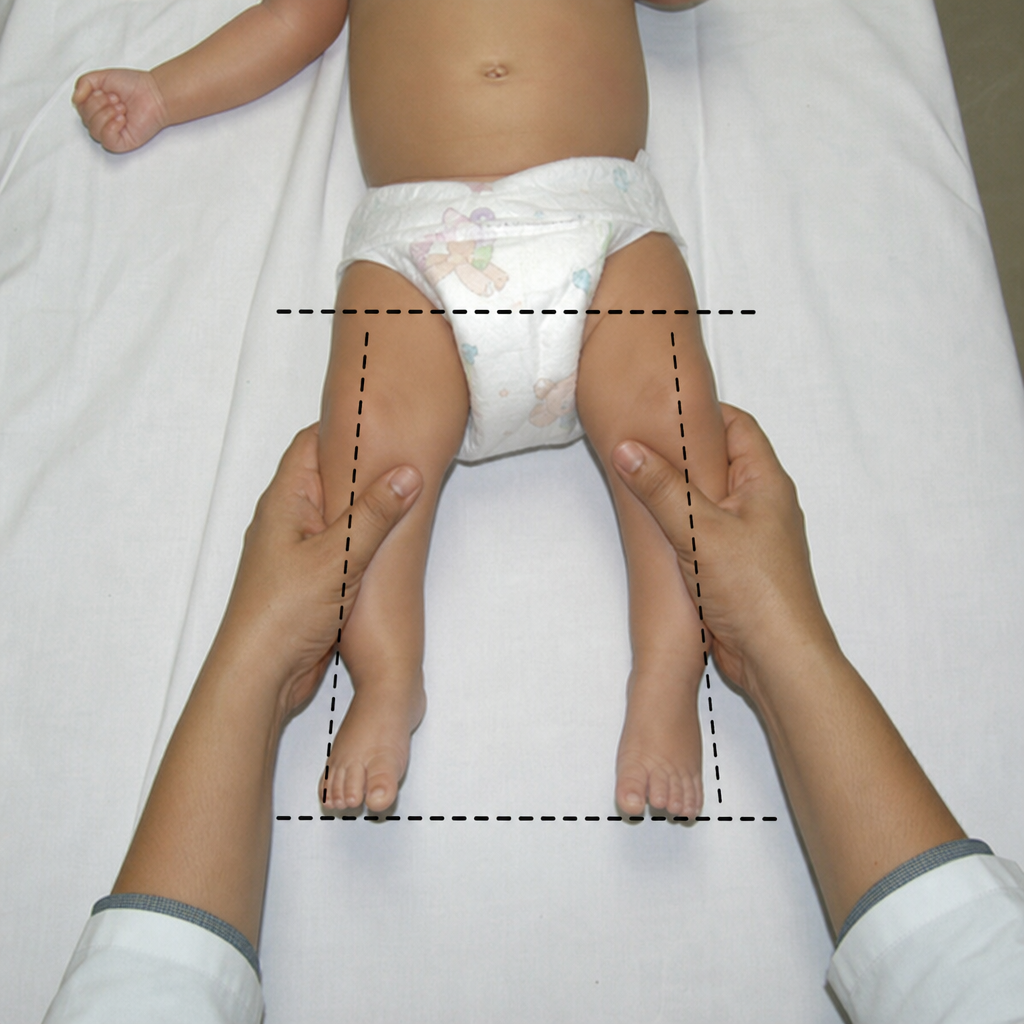
Which provocative test is used for the detection of developmental dysplasia of the hip (CDH)?
A 12-year-old child presents with tingling sensation and numbness in the little finger and gives a history of fracture in the elbow region 4 years back. What is the probable previous injury?
What is the spot diagnosis for a foot deformity described as a rocker bottom foot?
Siffert-Katz sign is seen in which of the following conditions?
Which physical examination maneuver is depicted?
Practice by Chapter
Developmental Dysplasia of Hip
Practice Questions
Clubfoot
Practice Questions
Pediatric Fractures
Practice Questions
Growth Plate Injuries
Practice Questions
Legg-Calvé-Perthes Disease
Practice Questions
Slipped Capital Femoral Epiphysis
Practice Questions
Pediatric Spine Deformities
Practice Questions
Cerebral Palsy: Orthopaedic Aspects
Practice Questions
Neuromuscular Disorders in Children
Practice Questions
Pediatric Bone and Joint Infections
Practice Questions
Limb Length Discrepancies
Practice Questions
Orthopedic Manifestations of Genetic Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app