
Orthopedic Biomechanics — MCQs

On this page
Which posture is associated with the greatest lumbar intradiscal pressure?
Which of the following muscles is primarily responsible for generating propulsive force during the push-off phase of normal gait?
What is the primary dynamic stabilizer of the patella against the lateral pull of the vastus lateralis?
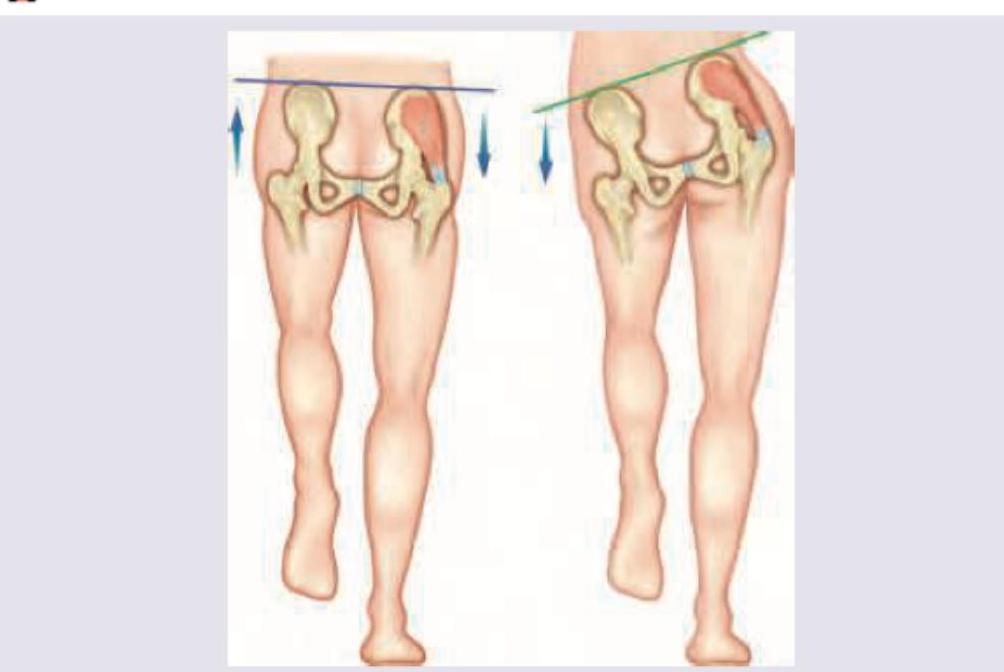
The following gait is seen due to weakness of:

The following gait is due to weakness of:
Following a road traffic accident, a patient develops type IIIa compound tibial fracture. Arrange the following external fixators in decreasing order of their stability (highest to lowest) 1. Ilizarov fixator 2. Uniplanar with a single rod 3. Uniplanar with double rod 4. Biplanar frame/Ring with a cylindrical rod
Trendelenburg sign is positive due to the involvement of:
Wolff's law is:-
During an autopsy, a pathologist finds a transverse fracture of the femur. Which type of force is most likely responsible for this fracture?
Increased Q angle predisposes to
Practice by Chapter
Principles of Biomechanics
Practice Questions
Biomechanics of Fracture Fixation
Practice Questions
Biomechanics of Spine
Practice Questions
Biomechanics of Hip
Practice Questions
Biomechanics of Knee
Practice Questions
Biomechanics of Foot and Ankle
Practice Questions
Biomechanics of Upper Limb
Practice Questions
Gait Analysis
Practice Questions
Biomechanics of Arthroplasty
Practice Questions
Biomechanics of Sports Injuries
Practice Questions
Computational Modeling in Orthopaedics
Practice Questions
Clinical Applications of Biomechanics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app