
Orthopaedic Techniques — MCQs

On this page
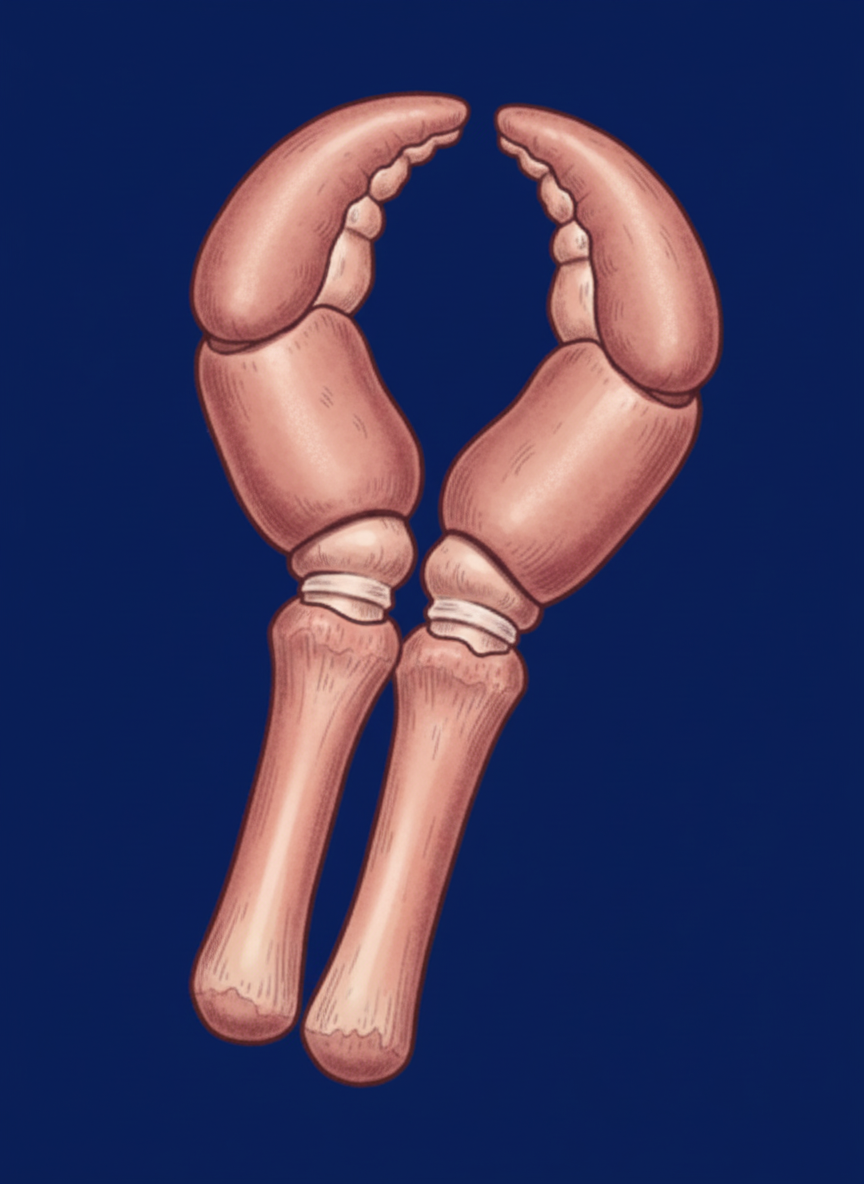
Which type of amputation is shown below?
The abduction contracture at the hip joint is evaluated clinically by which test?
In the surgical anterolateral approach to the tibia, why is the incision taken over the tibialis anterior muscle mass rather than over the shaft?
All of the following are principles of tendon transfers except?
What is the maximum tourniquet time for the upper limb?
What is the most important technical consideration at the time of performing a below-knee amputation?
In lag screw technique, what is the function of countersink?
Which of the following is the primary use of the instrument shown below?

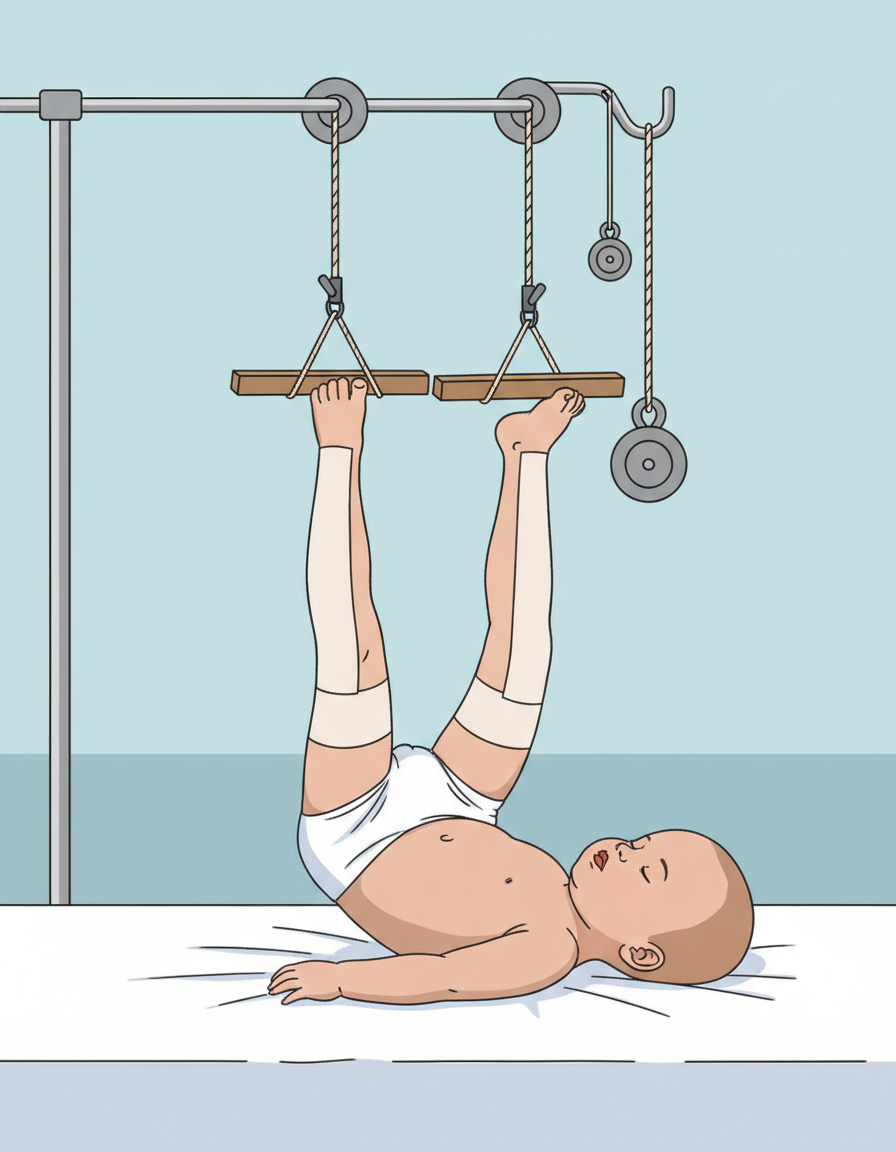
Which of the following describes the type of traction shown in the image?
Identify the splint shown in the image:

Practice by Chapter
Principles of Internal Fixation
Practice Questions
External Fixation
Practice Questions
Intramedullary Nailing
Practice Questions
Plate Osteosynthesis
Practice Questions
Tension Band Wiring
Practice Questions
Minimally Invasive Orthopaedic Surgery
Practice Questions
Arthroscopic Techniques
Practice Questions
Suture Techniques in Orthopaedics
Practice Questions
Navigation and Robotics
Practice Questions
3D Printing Applications
Practice Questions
Bone Grafting Techniques
Practice Questions
Local Flaps and Soft Tissue Coverage
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app