
Tumor-Like Conditions — MCQs

Most common site of myositis ossificans ?
Osteitis fibrosa cystica is associated with which of the following conditions?
Most common benign tumor of bone?
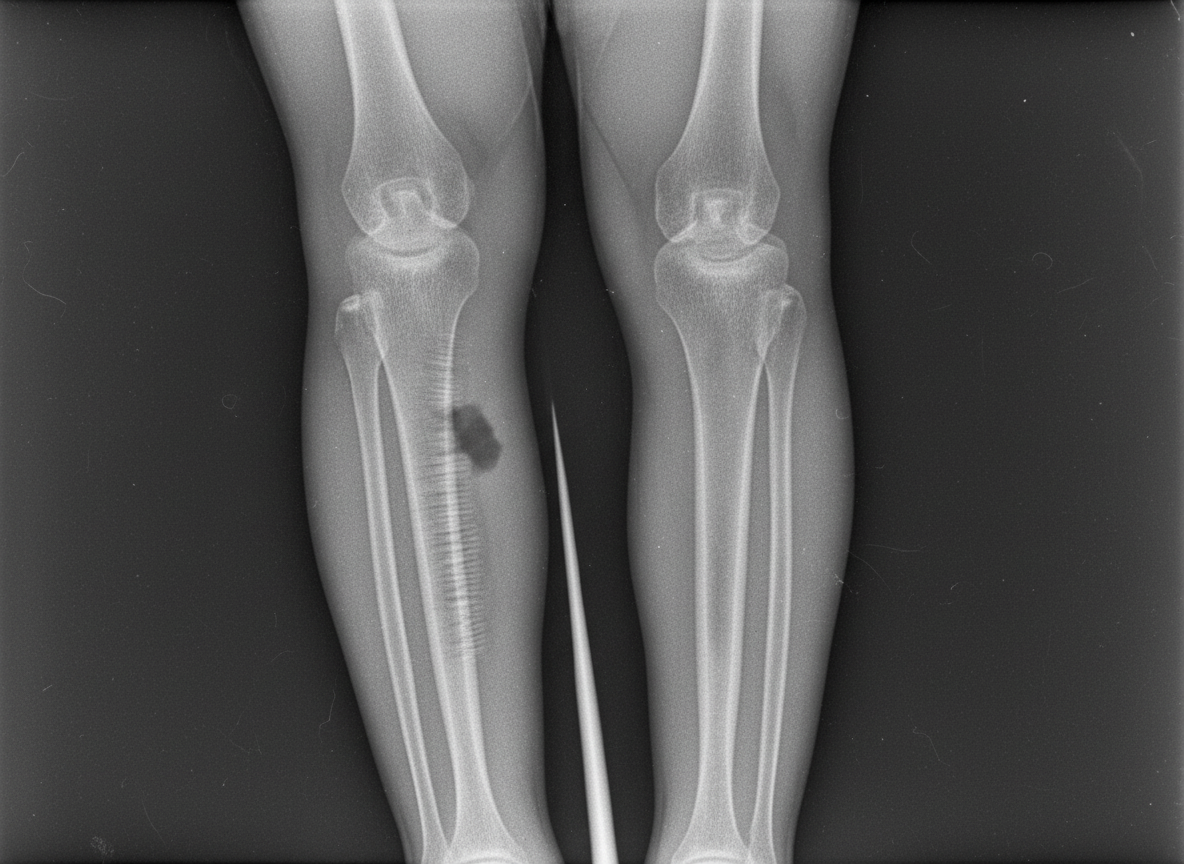
An 18-year-old boy presents with tenderness, warmth over the bone, and fever, ESR and CRP levels. The radiograph is shown below. What is the most likely diagnosis?
Following are seen in fibrous dysplasia EXCEPT
All of the following are features of myositis ossificans except -
Inspiratory stridor is found in what kind of lesions:
What is the most appropriate treatment for a soap bubble appearance at the lower end of the radius?
Most common site of osteogenic sarcoma is:
A 45 yrs male presented with an expansile lesion in the centre of femoral metaphysis. The lesion shows Endosteal scalloping and punctuate calcifications. Most likely diagnosis is:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app