
Metabolic Bone Diseases — MCQs

On this page
A 60-year-old person suffering from myositis ossificans progressive, what is the usual cause of death?
Which of the following are characteristic features of childhood osteopetrosis?
An X-ray of a patient shows bulbous ends of long bones, normal appositional bone growth, and failure of physiologic root resorption. Laboratory findings show myelophthisic anemia. What is the probable diagnosis?
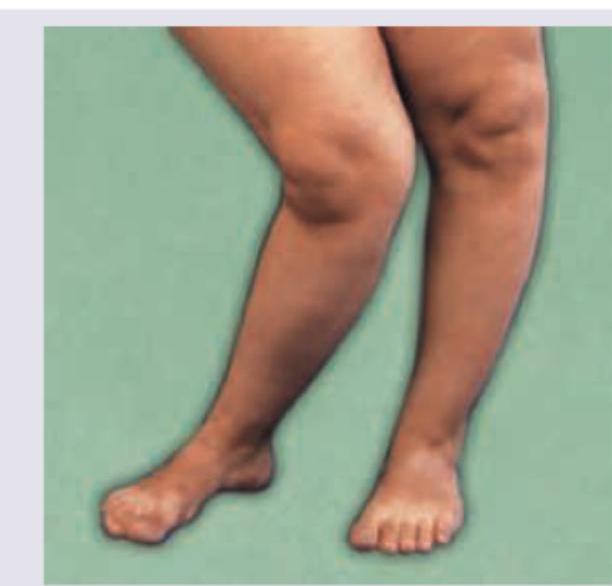
In a rural posting, a 35-year-old farmer comes to the OPD. Identify the condition shown:

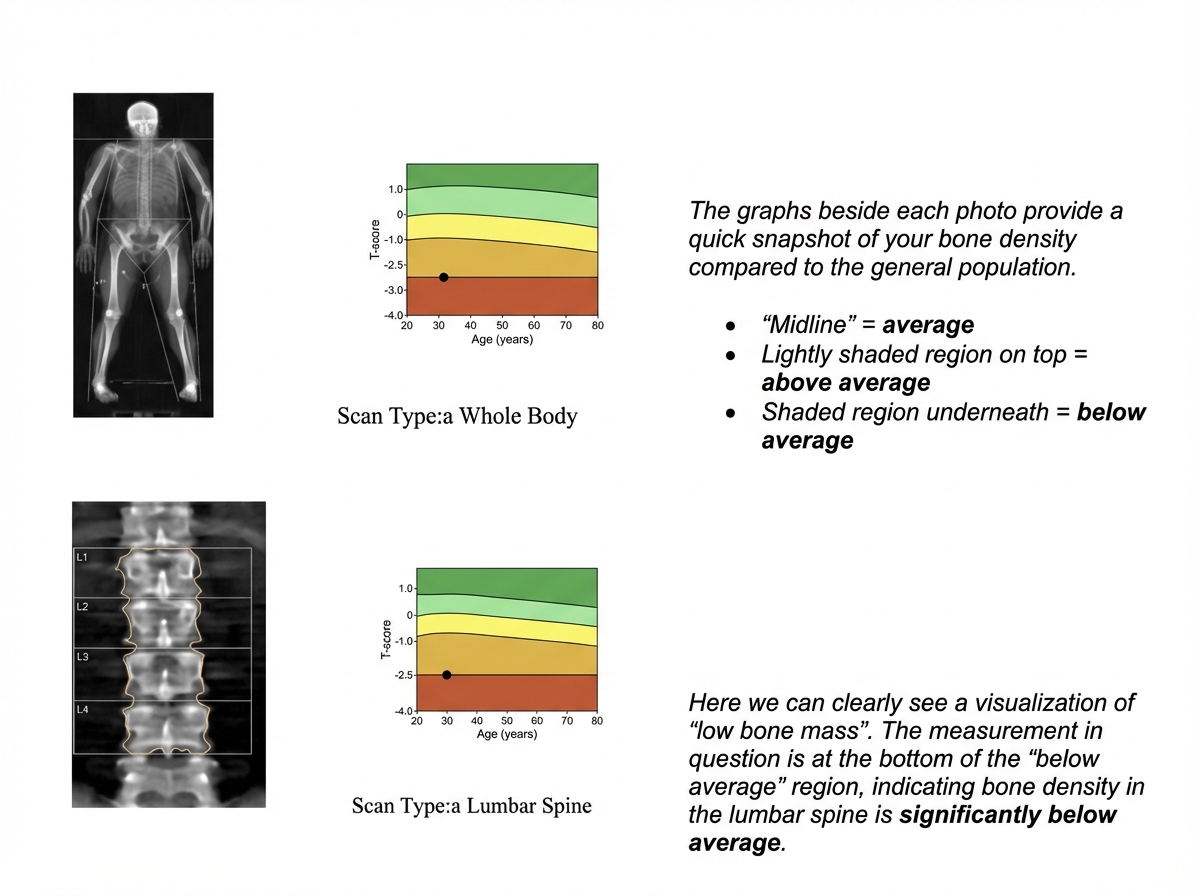
A 58-year-old postmenopausal woman undergoes bone densitometry. Which of the following is correct about the report shown?
A 72-year-old woman presents with bone pain and tenderness in her lower extremities and left clavicle. Laboratory studies reveal elevated calcium, decreased phosphate, and elevated serum alkaline phosphatase. X-ray spine shows?

Identify the deformity seen in this child with rickets:
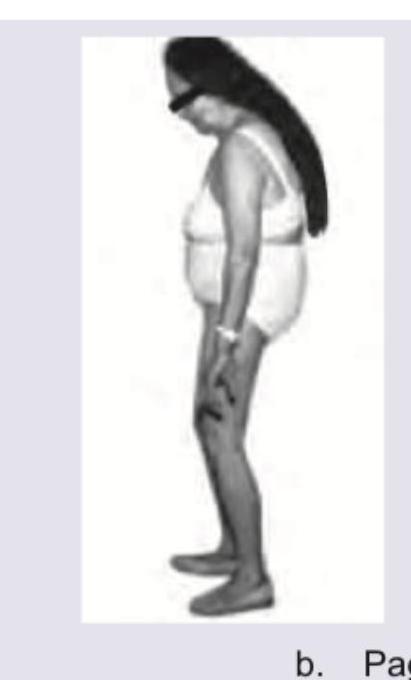
The appearance shown in the image is called as Simian Posturing. Notice the bent trunk, flexed legs and loss of spine normal axis. It occurs due to disordered bone turnover involving pelvis and vertebra. Which condition is most associated with this presentation?
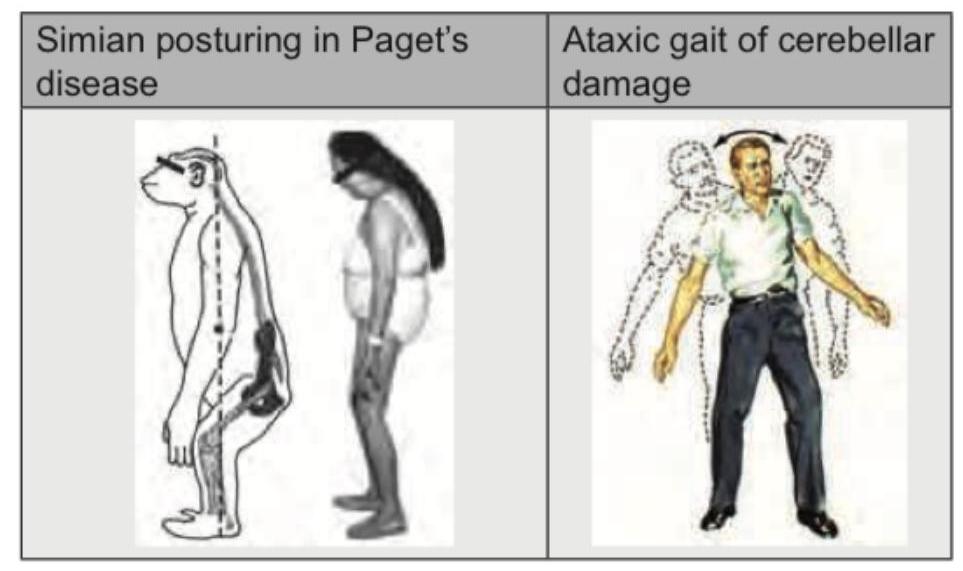
Which of the following diseases will lead to the following appearance?
A 60-year-old elderly female with a previous history of a Colles fracture is now complaining of backache. Which of the following statements regarding the treatment of this patient is incorrect?
Practice by Chapter
Osteoporosis
Practice Questions
Osteomalacia and Rickets
Practice Questions
Paget's Disease of Bone
Practice Questions
Hyperparathyroidism
Practice Questions
Renal Osteodystrophy
Practice Questions
Fluorosis
Practice Questions
Osteogenesis Imperfecta
Practice Questions
Bone Mineral Density Assessment
Practice Questions
Pharmacological Management of Metabolic Bone Diseases
Practice Questions
Surgical Considerations in Metabolic Bone Diseases
Practice Questions
Fragility Fractures
Practice Questions
Prevention Strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app