
Hand Surgery — MCQs

On this page
Dupuytren's contracture is associated with which of the following conditions?
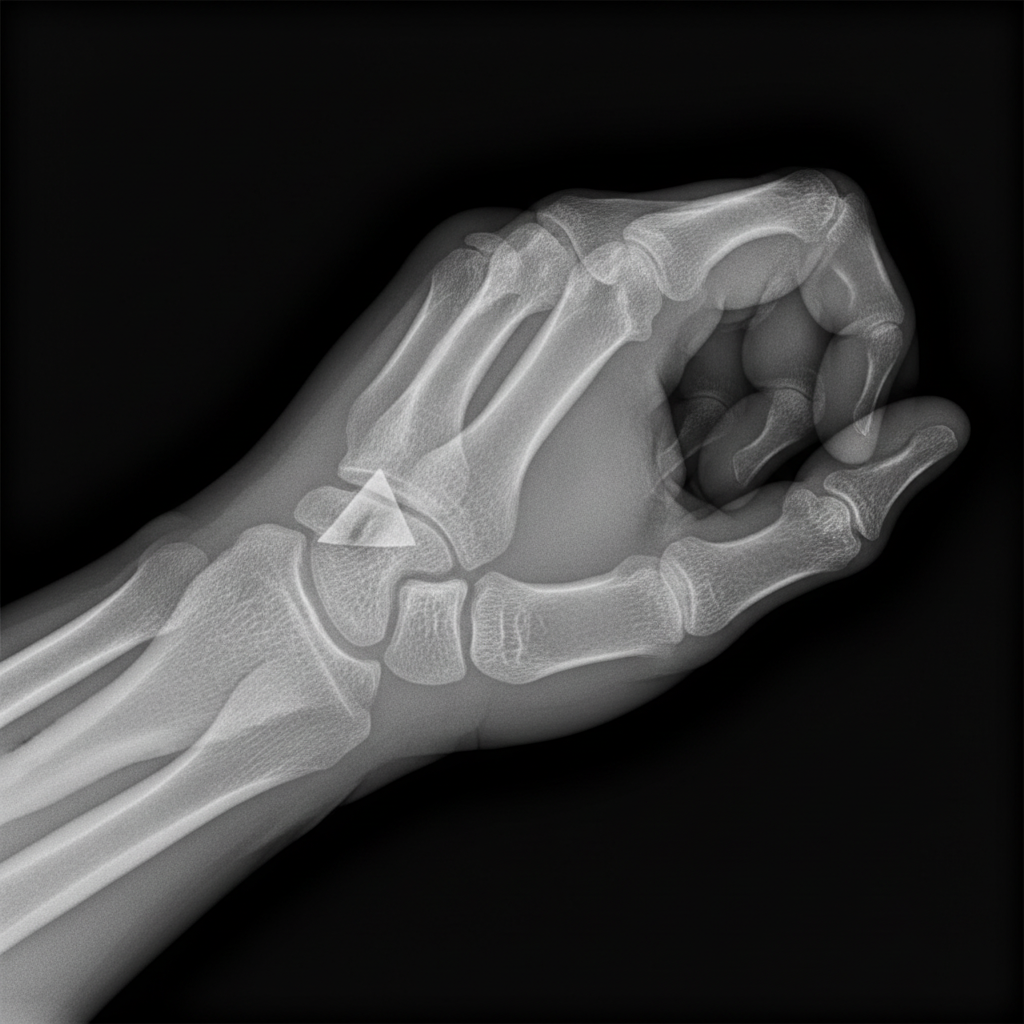
Fracture shown in this radiograph is:
Which of the following scaphoid fractures is most prone to develop avascular necrosis?
Which of the following statements is FALSE regarding radial club hand?
A 19-year-old boy has a history of falling on an outstretched hand while playing. He developed slight radial side pain and tenderness. On examination, pressure along the axis of the thumb is painful, and X-rays are normal. What is the most likely diagnosis?
Dupuytren's contracture commonly affects which finger?
Which of the following statements about nerve entrapment syndromes is FALSE?
Which of the following tests is known for assessing De Quervain's tenosynovitis?
Which of the following is NOT a cause of carpal tunnel syndrome?
Which of the following diagnostic studies is NOT useful in the evaluation of upper-extremity pain?
Practice by Chapter
Hand Anatomy and Biomechanics
Practice Questions
Hand Fractures and Dislocations
Practice Questions
Tendon Injuries
Practice Questions
Nerve Injuries in Hand
Practice Questions
Dupuytren's Disease
Practice Questions
Carpal Tunnel Syndrome
Practice Questions
Rheumatoid Hand
Practice Questions
Reconstructive Hand Surgery
Practice Questions
Tendon Transfers
Practice Questions
Congenital Hand Anomalies
Practice Questions
Hand Infections
Practice Questions
Microsurgery in Hand Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app