
Hand Surgery — MCQs

On this page
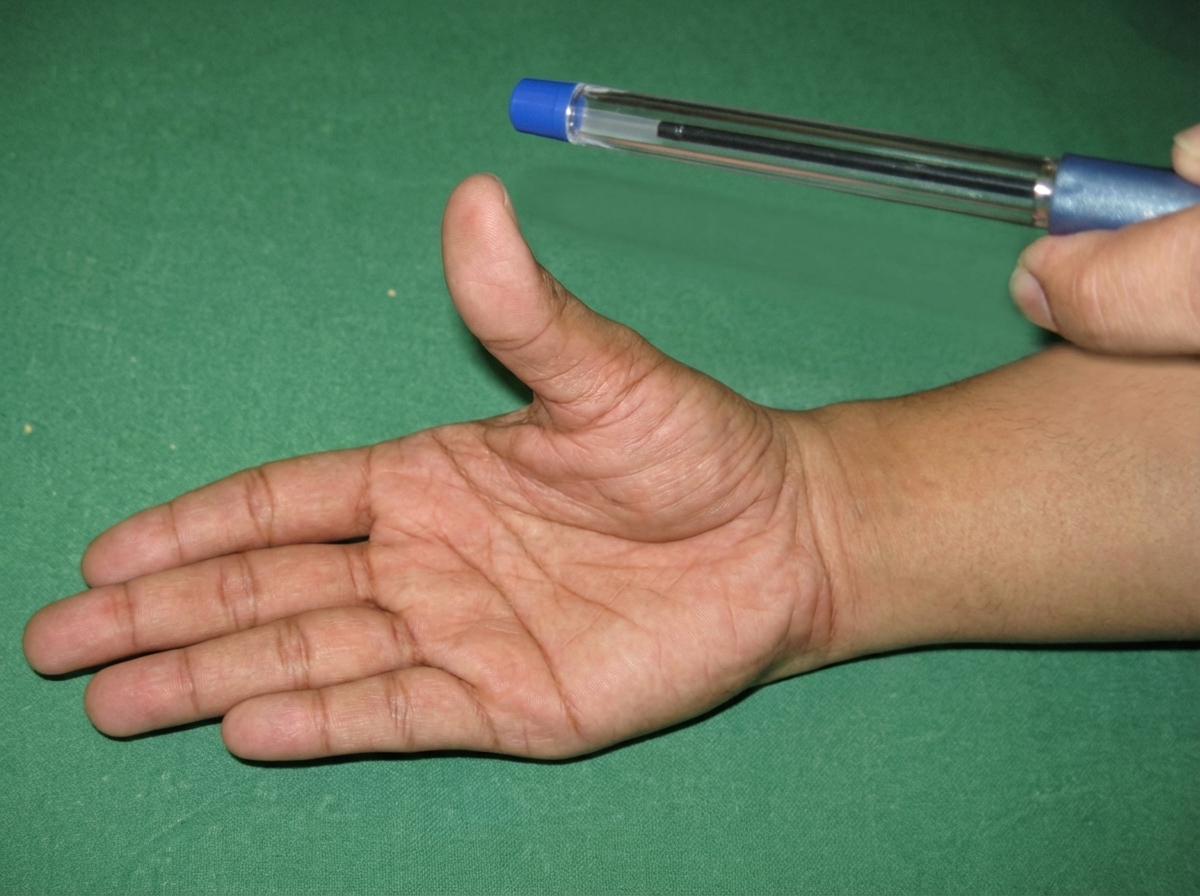
Which nerve injury is elicited by the 'pen test'?
A 35-year-old right-handed construction worker presents with complaints of nocturnal numbness and pain involving the right hand. Symptoms wake him and are then relieved by shaking his hand. There is some atrophy of the thenar eminence. Tinel sign is positive. What is the best advice for this patient?
Cubital tunnel syndrome involves which nerve?
Trigger finger is commonly associated with which of the following conditions?
Kanavel's sign is seen in?
What test is being performed?

A 35-year-old construction worker presents with complaints of nocturnal paresthesias of the thumb, index, and middle fingers. There is some atrophy of the thenar eminence. Tinel's sign is positive. What is the most likely diagnosis?
The test performed below shows involvement of which of the following nerve?
A 69-year-old man presents with numbness in the middle three digits of his right hand and difficulty grasping objects. He has a history of 50 years as a carpenter and has atrophy of the thenar eminence. What is the most likely cause of his hand problems?
Froment's sign is due to injury of which nerve?
Practice by Chapter
Hand Anatomy and Biomechanics
Practice Questions
Hand Fractures and Dislocations
Practice Questions
Tendon Injuries
Practice Questions
Nerve Injuries in Hand
Practice Questions
Dupuytren's Disease
Practice Questions
Carpal Tunnel Syndrome
Practice Questions
Rheumatoid Hand
Practice Questions
Reconstructive Hand Surgery
Practice Questions
Tendon Transfers
Practice Questions
Congenital Hand Anomalies
Practice Questions
Hand Infections
Practice Questions
Microsurgery in Hand Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app