
Hand Surgery — MCQs

On this page
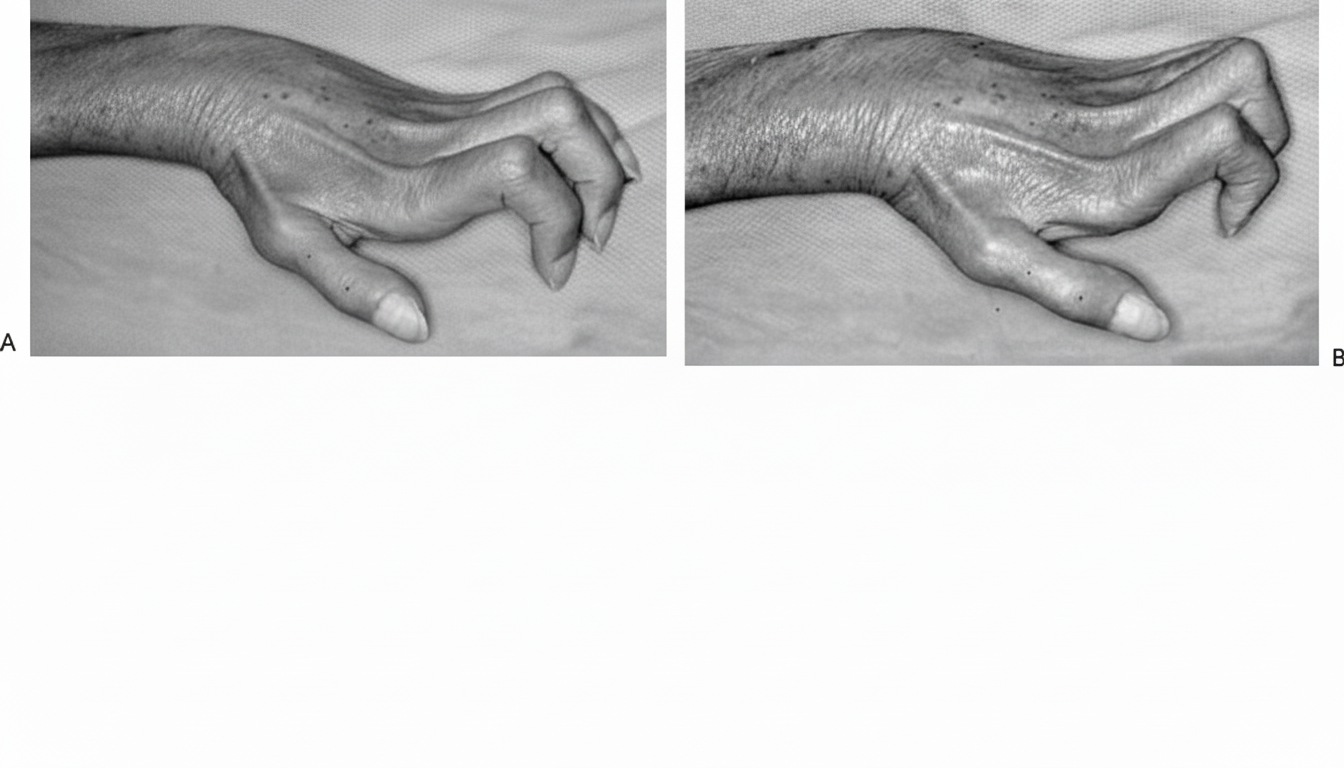
What is this condition known as?

A 57-year-old woman presents with numbness and tingling in her right thumb, index, and long finger for the past four weeks. She reports waking up in the middle of the night with these symptoms, requiring her to shake her hands to alleviate them. She denies similar symptoms in her other hand or legs and has no neck or upper arm pain. Physical examination reveals that her symptoms are reproduced by Tinel testing and exacerbated by wrist hyperflexion. Decreased sensation is noted over the palmar aspects of the thumb, index, and middle fingers, with no apparent motor weakness. What is the most likely diagnosis?
Carpal tunnel syndrome is associated with all of the following except:
Carpal tunnel syndrome is caused by all of the following conditions EXCEPT?
A patient presented with a history of fall on an outstretched hand. There is pain and swelling over the radial aspect of the wrist without any obvious deformity. The radial styloid process is at a lower level than the ulnar styloid process. Tenderness can be elicited in the anatomical snuff box. Which of the following is the most likely diagnosis?
A boxer's fracture is a fracture through which part of the bone?
Which splint is used for the condition shown below?
Which test is demonstrated in the image?

A patient is unable to actively extend the terminal phalange, although the distal interphalangeal joint can be extended passively. What is this condition known as?
A 40-year-old diabetic man presents with an inability to bend his ring finger and small nodules on the palm. Which of the following would NOT be part of your management for this patient?
Practice by Chapter
Hand Anatomy and Biomechanics
Practice Questions
Hand Fractures and Dislocations
Practice Questions
Tendon Injuries
Practice Questions
Nerve Injuries in Hand
Practice Questions
Dupuytren's Disease
Practice Questions
Carpal Tunnel Syndrome
Practice Questions
Rheumatoid Hand
Practice Questions
Reconstructive Hand Surgery
Practice Questions
Tendon Transfers
Practice Questions
Congenital Hand Anomalies
Practice Questions
Hand Infections
Practice Questions
Microsurgery in Hand Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app