
Hand Surgery — MCQs

On this page
Which action is affected in Bennet's fracture of the thumb?
Which of the following is seen in Boutonniere's deformity?
The term Bennett's fracture is used to describe which of the following?
Which of the following is the most appropriate diagnosis for a patient presenting with wrist pain and stiffness, especially after repetitive stress, with a characteristic "humpback" deformity?
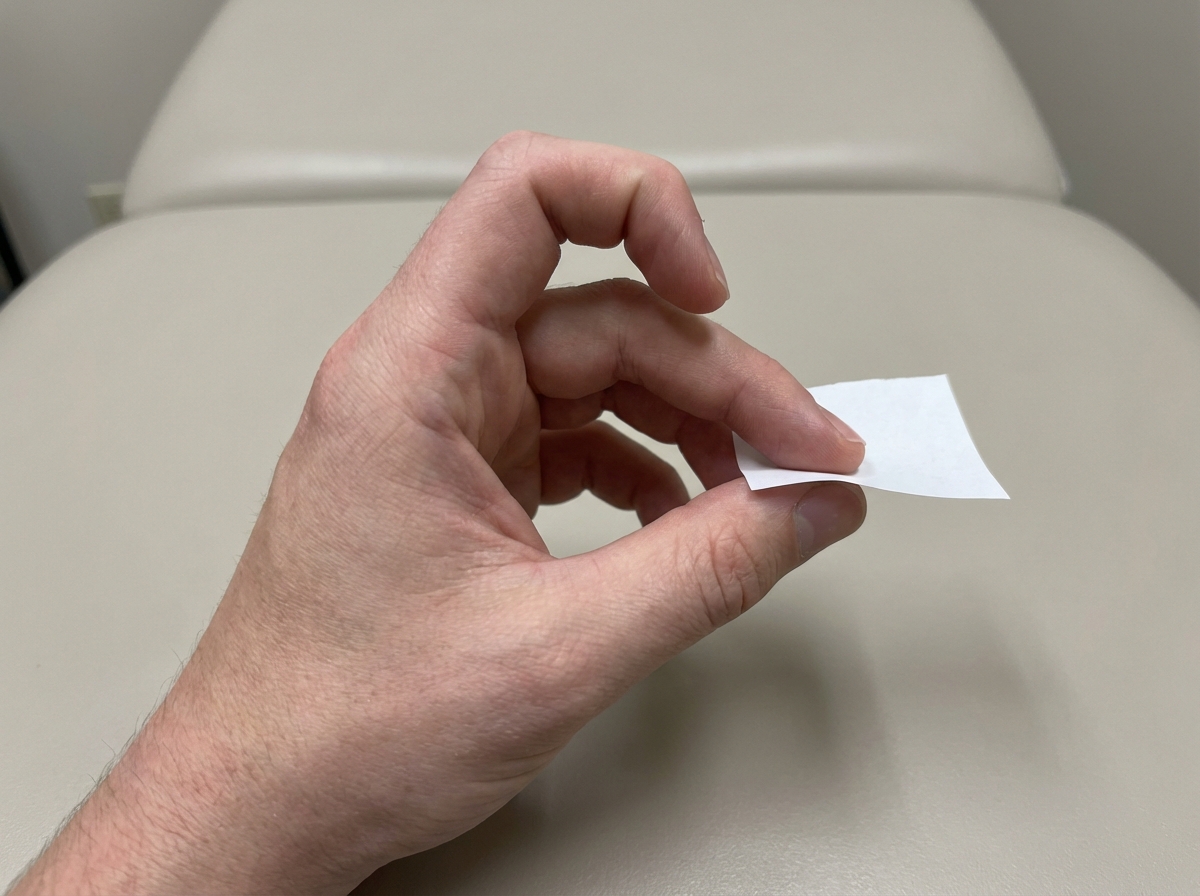
Which nerve palsy is diagnosed using this test?
A middle-aged female presents with pain and tenderness at the base of the thumb, with a history of chronic wrist overuse. A specific maneuver, involving making a fist with the thumb inside and then bending the wrist towards the little finger, elicits pain. Which two tendons are primarily involved in this condition?
Which of the following statements is NOT TRUE regarding Dupuytren's contracture?
Claw hand is seen in all conditions except?
A 66-year-old diabetic lady complains of pain in the palm of her right hand at the base of her ring finger, which is held in flexion. Extension is painful, produces an audible click, and often requires the assistance of the other hand. What is the first-line treatment for this condition?
What does Tinel's test assess?
Practice by Chapter
Hand Anatomy and Biomechanics
Practice Questions
Hand Fractures and Dislocations
Practice Questions
Tendon Injuries
Practice Questions
Nerve Injuries in Hand
Practice Questions
Dupuytren's Disease
Practice Questions
Carpal Tunnel Syndrome
Practice Questions
Rheumatoid Hand
Practice Questions
Reconstructive Hand Surgery
Practice Questions
Tendon Transfers
Practice Questions
Congenital Hand Anomalies
Practice Questions
Hand Infections
Practice Questions
Microsurgery in Hand Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app