
Hand Surgery — MCQs

On this page
X-ray of hand of the picture shows:

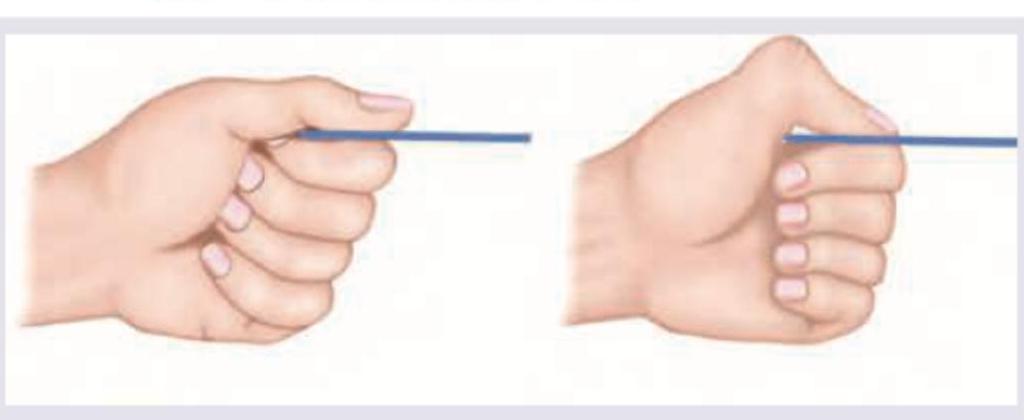
The test performed below shows involvement of which of the following nerve?
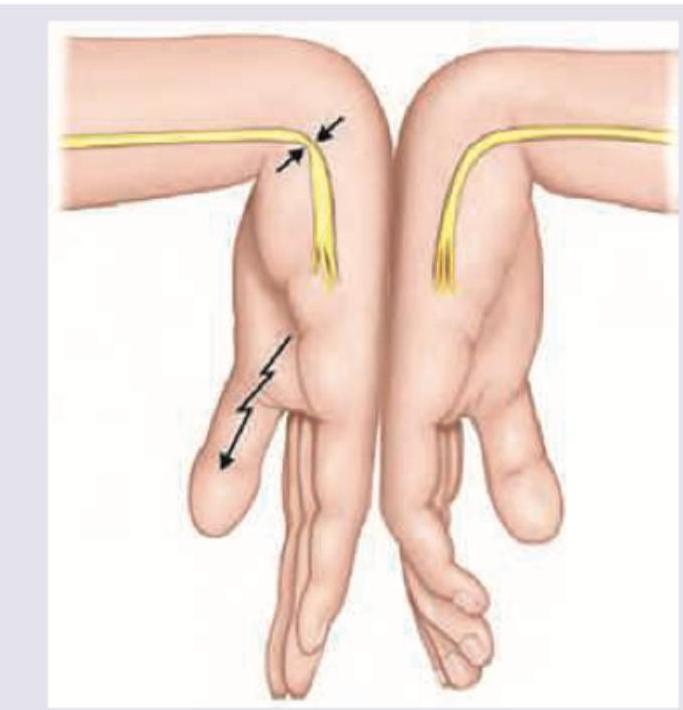
The test performed below shows involvement of which of the following nerve?
The contracture shown in the image is associated with all except:

A 35-year-old male comes with a swollen finger. A few days ago he got a cut on his index finger. The swelling has worsened with the development of redness. He also feels feverish. All of the following clinical features are correct about the diagnosis except:

The given nature of injury will lead to the development of:
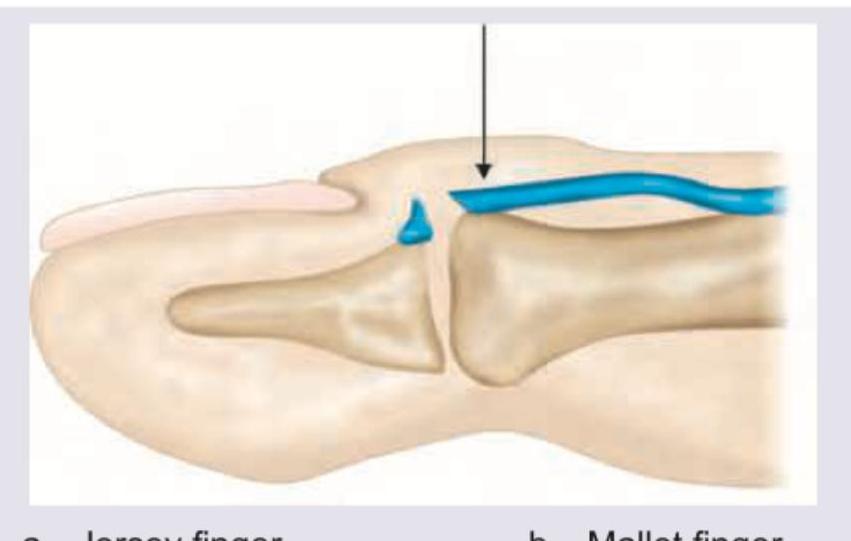
What does the following image show?

What is correct about the fracture shown in the figure?

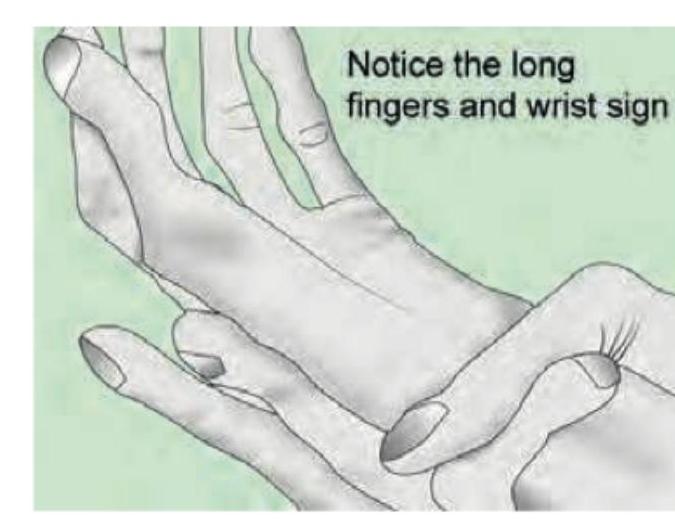
Identify the deformity:
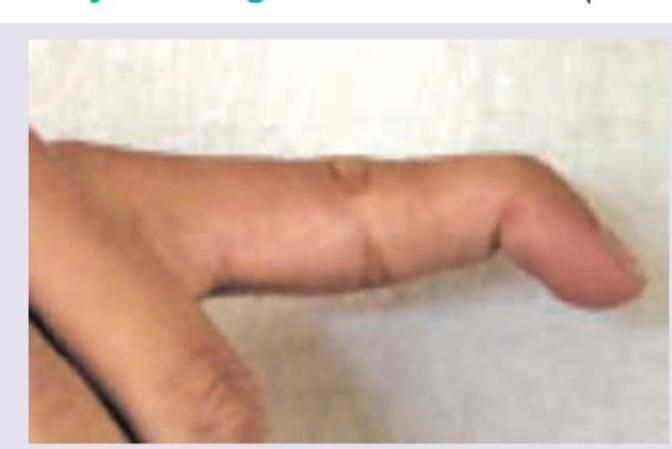
The image shows a characteristic finger deformity. What is the most likely diagnosis?
Practice by Chapter
Hand Anatomy and Biomechanics
Practice Questions
Hand Fractures and Dislocations
Practice Questions
Tendon Injuries
Practice Questions
Nerve Injuries in Hand
Practice Questions
Dupuytren's Disease
Practice Questions
Carpal Tunnel Syndrome
Practice Questions
Rheumatoid Hand
Practice Questions
Reconstructive Hand Surgery
Practice Questions
Tendon Transfers
Practice Questions
Congenital Hand Anomalies
Practice Questions
Hand Infections
Practice Questions
Microsurgery in Hand Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app