
Hand Surgery — MCQs

On this page
A patient experienced a fall onto an outstretched hand, and an X-ray revealed a fracture of the base of the first metacarpal with accompanying subluxation at the carpometacarpal (CMC) joint. Define this type of fracture.
Which nerve will be involved in the following finding at rest?
A teenager presents to the emergency department with wrist pain after falling off his skateboard. He has snuff-box tenderness. Which bone is likely fractured?
A labourer falls on an outstretched hand and complains of pain in the anatomical snuff box. Which of the following is the most appropriate next step?
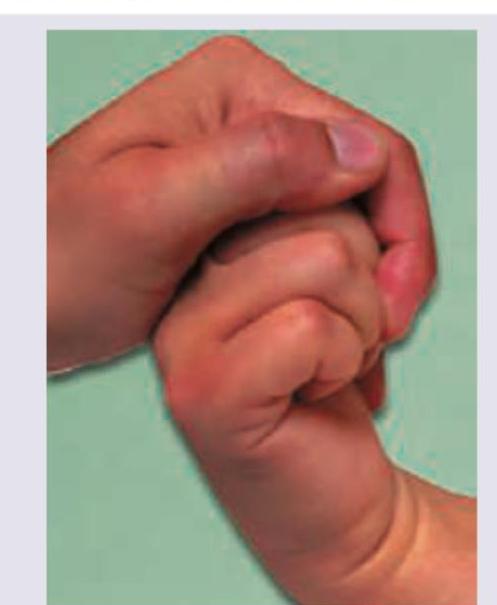
Identify the test being performed.
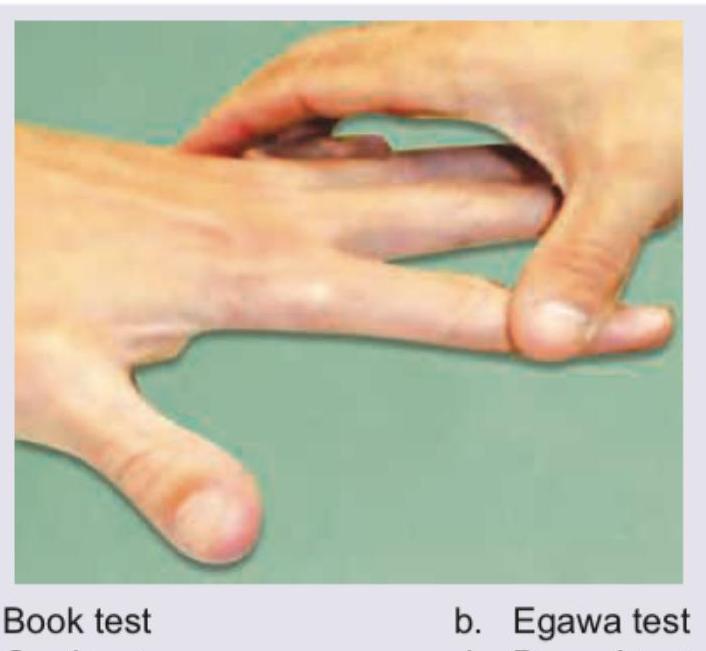
The test is performed for palsy of:

What is Incorrect about the test being performed?

The deformity shown below can be due to involvement of: (AIIMS May 2016)

Identify the true statement regarding the clinical examination given in the image:
The following test is done to elicit:

Practice by Chapter
Hand Anatomy and Biomechanics
Practice Questions
Hand Fractures and Dislocations
Practice Questions
Tendon Injuries
Practice Questions
Nerve Injuries in Hand
Practice Questions
Dupuytren's Disease
Practice Questions
Carpal Tunnel Syndrome
Practice Questions
Rheumatoid Hand
Practice Questions
Reconstructive Hand Surgery
Practice Questions
Tendon Transfers
Practice Questions
Congenital Hand Anomalies
Practice Questions
Hand Infections
Practice Questions
Microsurgery in Hand Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app