
Foot and Ankle Surgery — MCQs

On this page
Avascular necrosis is commoner in which of the following bones?
Which mechanism of injury is most commonly associated with ankle joint injuries?
A 32-year-old active male presents to the emergency department following a laceration to the posterior ankle sustained from a glass injury. On examination, there is a visible wound over the Achilles tendon region, he is unable to plantarflex the foot, and the Thompson test is positive. What is the treatment for this condition?

Bohler's angle is measured in fractures involving which tarsal bone?
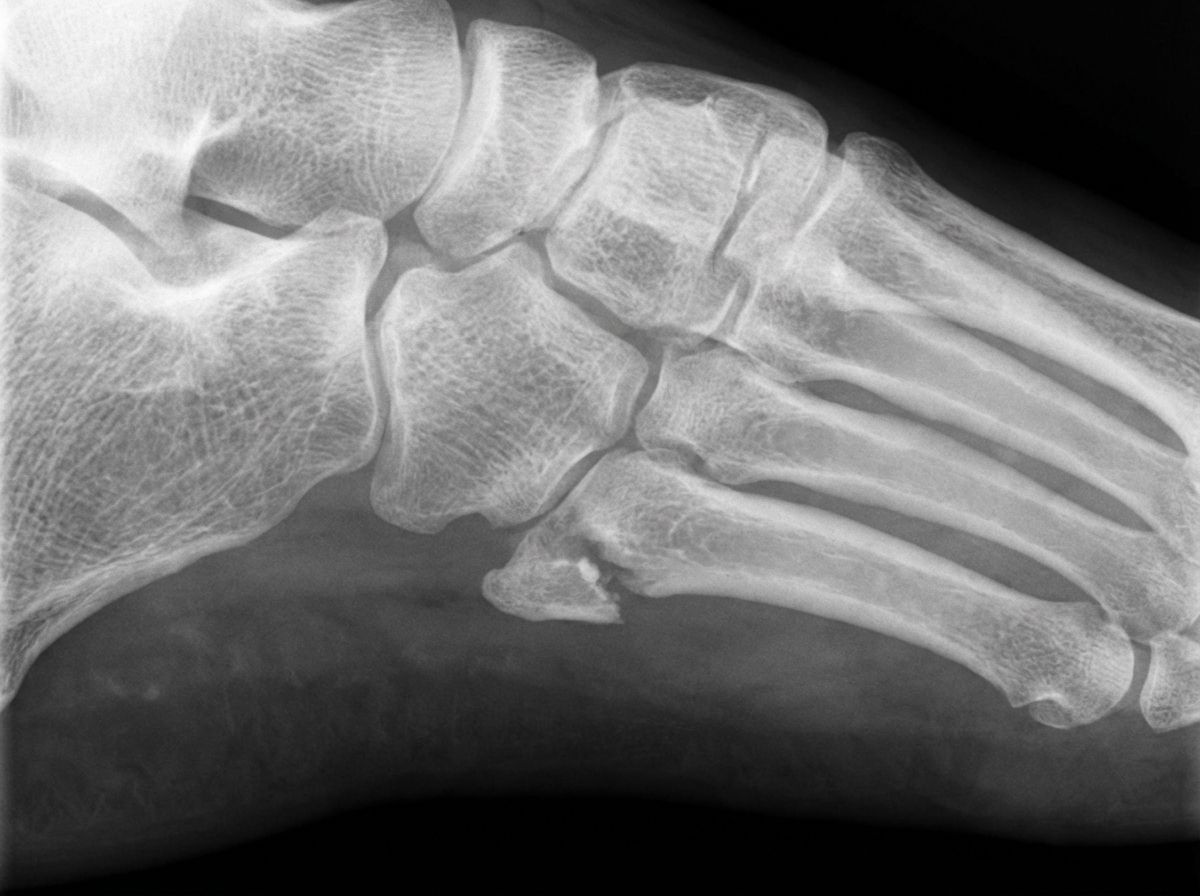
A 45-year-old male presents with foot pain after an injury. What is the mechanism of injury associated with the pathology seen in this X-ray?
Hallux valgus is associated with all of the following except:
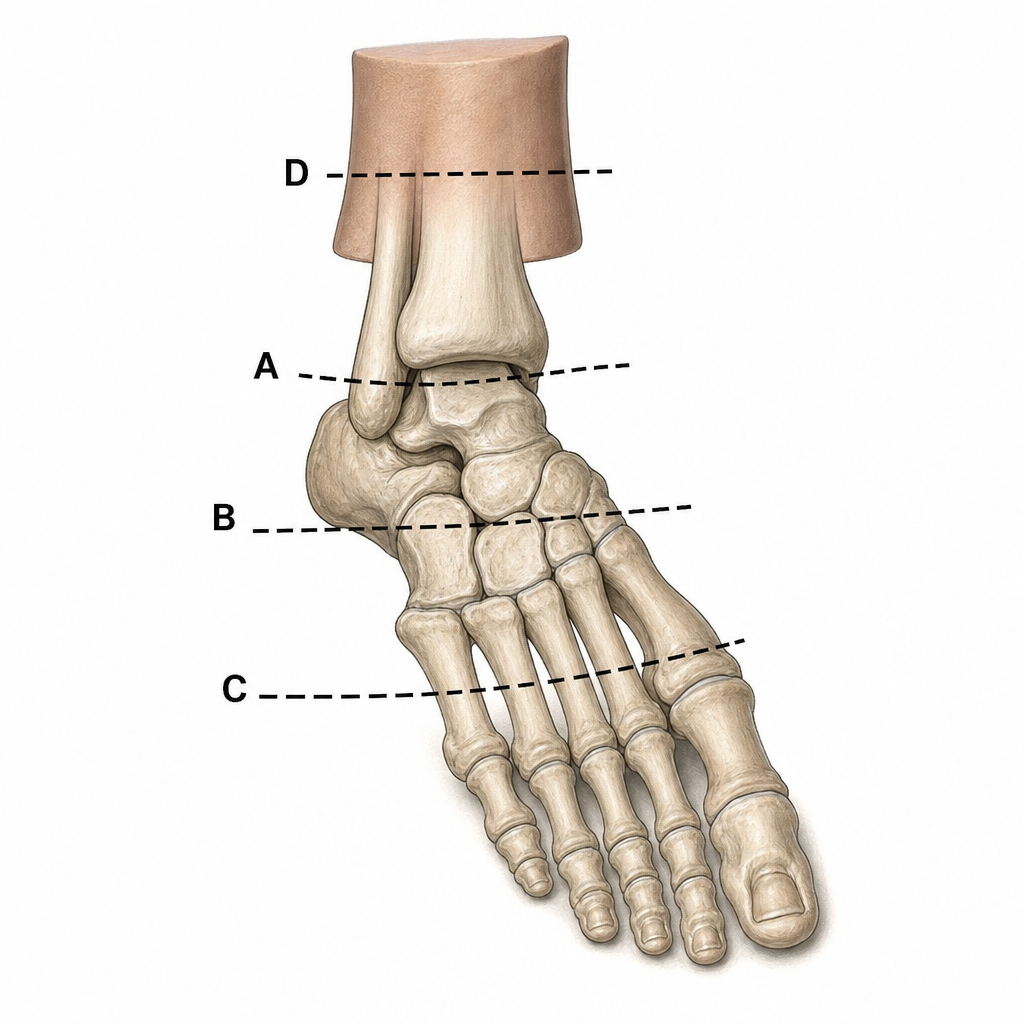
Amputation marked at level of 'C' is:
A 32-year-old athlete presents with posterior heel pain. Which of the following could be a differential diagnosis?
What is the optimal position of the ankle to prevent ankylosis?
The Hawkins Classification is used for which type of fracture?
Practice by Chapter
Foot and Ankle Anatomy
Practice Questions
Hallux Valgus
Practice Questions
Flatfoot Deformities
Practice Questions
Cavus Foot
Practice Questions
Ankle Instability and Sprains
Practice Questions
Achilles Tendon Disorders
Practice Questions
Diabetic Foot
Practice Questions
Foot and Ankle Arthritis
Practice Questions
Ankle Fractures
Practice Questions
Foot Fractures
Practice Questions
Tendon Disorders of Foot and Ankle
Practice Questions
Reconstructive Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app