
Ankle Fractures — MCQs

An RTA patient presented to the emergency department with severe pain in the ankle. An X-ray was performed, given below. What is the best next step in management?

A ballet dancer presents with chronic anterolateral ankle pain. Most likely diagnosis?
The operative procedure known as "microfracture" is done for the
Immediate treatment of compound fracture of tibia includes:
Commonest ligament injured in ankle injury ?
All of the following are indications for open reduction and internal fixation (ORIF) of fractures EXCEPT:
The rephrased question is:What is the most common complication of a fractured talus?
A 10-year-old obese boy was referred to the emergency department with a history of hip pain. He was observed to be limping and complained of severe pain. Which of the following investigations is least appropriate for this condition?
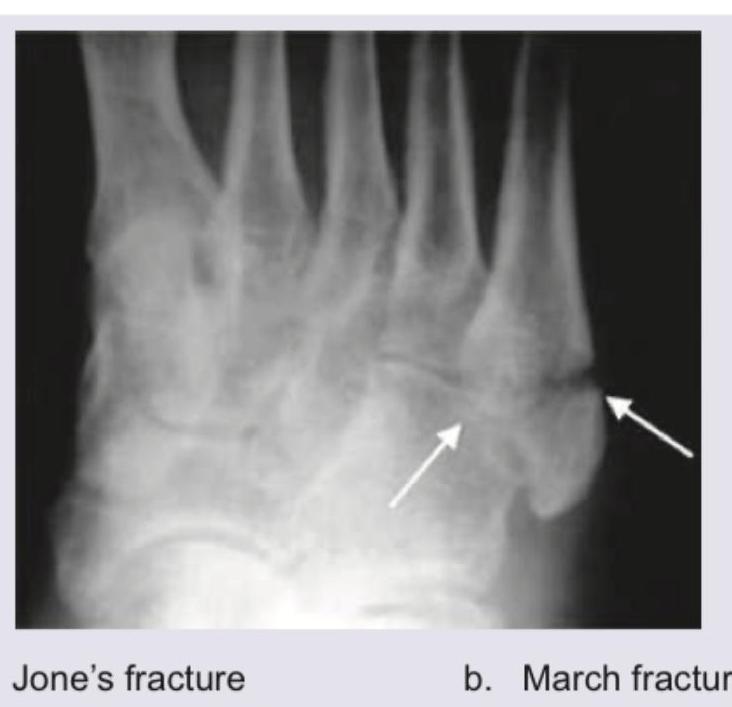
Comment on the diagnosis:
Match List-I with List-II and select the correct answer using the code given below the Lists: **List-I** A. Atrial fibrillation B. Ventricular tachycardia C. Complete heart block D. Ventricular fibrillation **List-II** 1. Chaotic rhythm 2. Dissociation of P and QRS waves 3. Wide QRS complexes and regular rapid rate 4. Irregular R-R interval without P waves
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app