
Future Trends in Computer-Assisted Orthopaedics — MCQs

What is the condition commonly known as jumper's knee?
Gold standard investigation for breast carcinoma screening in a patient with silicone breast implants
In which of the following situations is breast conservation surgery not indicated?
All of the following are indications for open reduction and internal fixation (ORIF) of fractures EXCEPT:
Which technique is considered the best for evaluating bone regeneration after periodontal surgery?
Vacuum assisted closure is contraindicated in which of the following conditions -
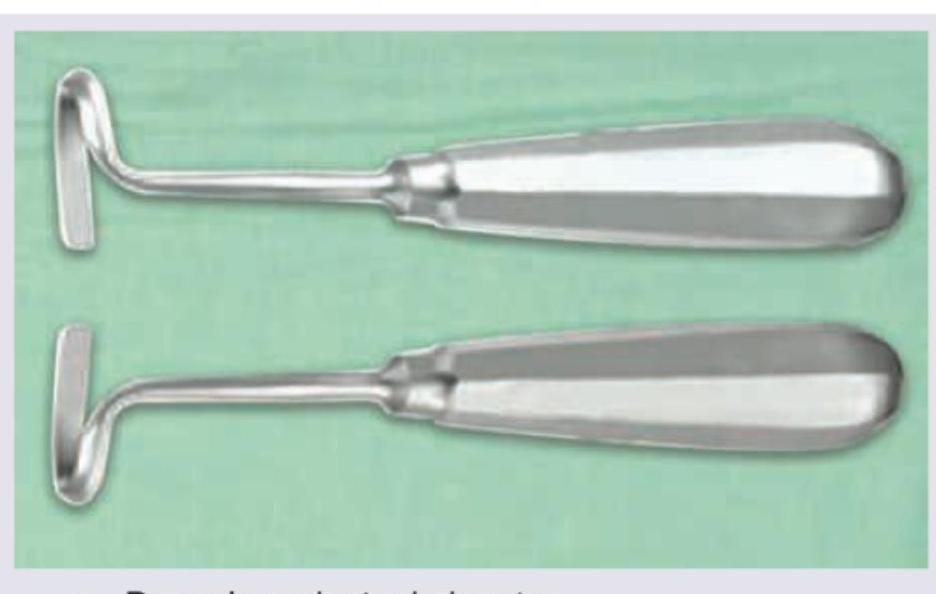
What does the given image show?
A surgeon experiences pin-site fracture during reference array fixation in computer-navigated TKA in an osteoporotic patient. Subsequently, three more cases develop similar complications. What systematic approach should be implemented to prevent this complication?
A tertiary care center is planning to implement computer-assisted surgery program for joint replacement. They have limited budget and expertise. Which factor should be prioritized when selecting a navigation system?
A study compares outcomes of computer-navigated versus conventional total knee arthroplasty. Navigation group shows 95% implants within 3 degrees of neutral mechanical axis versus 80% in conventional group (p<0.05). However, 5-year functional outcomes and survival rates are similar. What is the most appropriate interpretation?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app