
Surveillance and Follow-up — MCQs

Which of the following is not true about osteosarcoma?
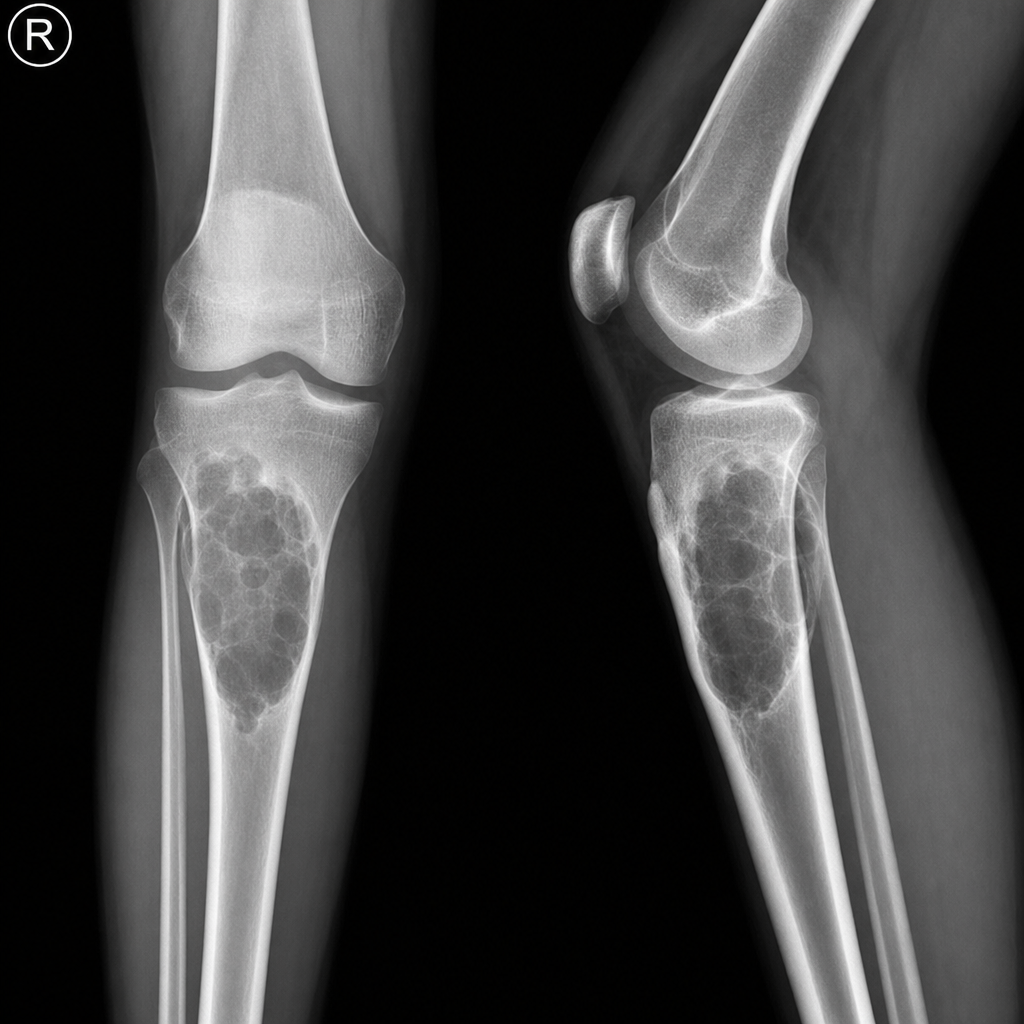
Following X-ray shows the most probable diagnosis as?
Distant bone metastases can be best detected by which of the following imaging techniques?
What is the average time interval between radiation exposure and genesis of post-radiation osteosarcoma?
What is the significance of a 2-year post-treatment surveillance period in paucibacillary leprosy?
A 45 yrs male presented with an expansile lesion in the centre of femoral metaphysis. The lesion shows Endosteal scalloping and punctuate calcifications. Most likely diagnosis is:
Most common site of osteogenic sarcoma is:
A 28-year-old female presents to the clinic with a complaint of dull, aching pain in her left hand after accidentally striking her finger against a door frame. On physical examination, there is mild tenderness over the affected area, but the range of m otion is preserved. An X -ray of the hand is shown below. Based on the clinical presentation and radiographic findings, what is the most likely diagnosis?
A 9-year-old child presents with pain and swelling over the mid -shaft of the tibia, associated with low -grade fever and an elevated erythrocyte sedimentation rate (ESR). An X-ray of the affected limb is shown below. Based on the clinical features and radiographic findings, what is the most likely diagnosis?
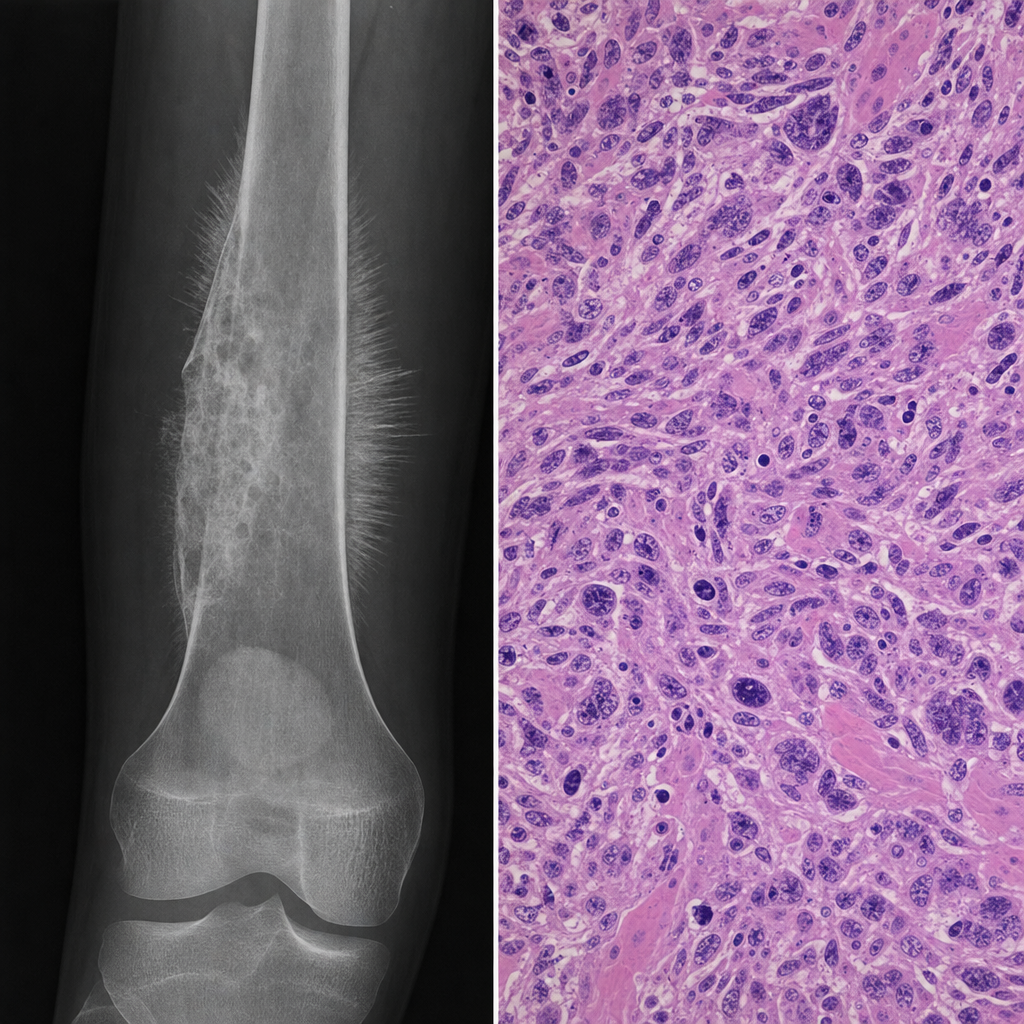
A 16-year-old boy presents with a 3-month history of progressively worsening pain and swelling around the distal right femur. Plain radiograph shows a permeative lytic lesion with Codman's triangle and a sunburst periosteal reaction. A core needle biopsy is performed and the histopathological specimen is shown in Image 1. Following staging workup, imaging confirms the lesion is confined to the bone with no skip lesions and no distant metastases. What is the most appropriate next step in management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app