
Bone Tumors — MCQs

On this page
What condition is characterized by the presence of a nidus?
A 20-year-old patient presents with a sclerotic lesion at the diaphysis. What is the most likely diagnosis?
Mazabraud syndrome is characterized by which of the following?
What is the most common malignant bone tumor?
A 15-year-old boy presented with painful swelling over the left shoulder. Radiograph of the shoulder showed an osteolytic area with stippled calcification over the proximal humeral epiphysis. Biopsy of the lesion revealed an immature fibrous matrix with scattered giant cells. What is the most likely diagnosis?
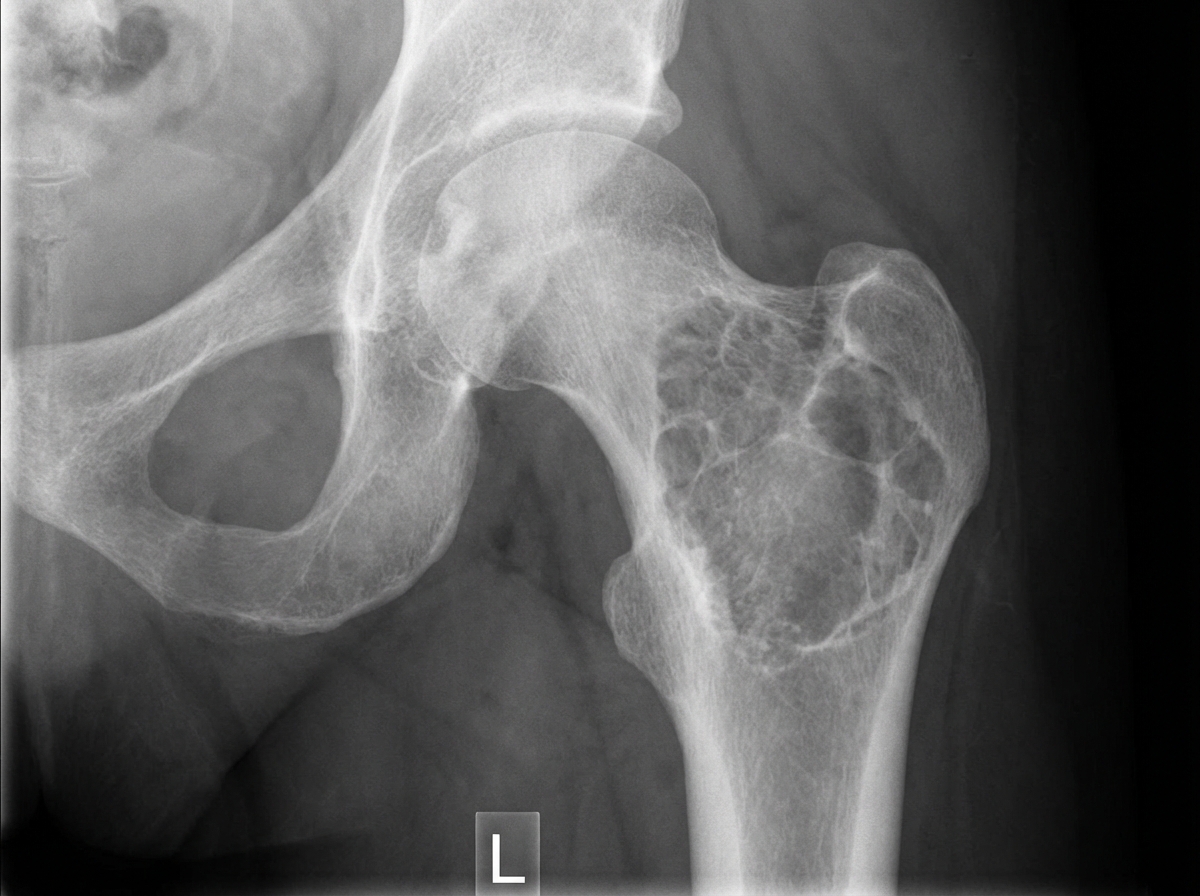
A 30-year-old male presented with hip pain for the last 6 months. A hip X-ray is provided. What is the likely diagnosis?
What is true about Ameloblastoma?
Which of the following tumors is associated with raised serum alkaline phosphatase levels?
What is the standard surgical staging system for bone tumors?
A patient with which of the following diseases is predisposed to develop osteosarcoma?
Practice by Chapter
Classification of Bone Tumors
Practice Questions
Benign Bone Tumors
Practice Questions
Malignant Primary Bone Tumors
Practice Questions
Metastatic Bone Disease
Practice Questions
Tumor-Like Lesions of Bone
Practice Questions
Soft Tissue Tumors
Practice Questions
Evaluation and Staging of Bone Tumors
Practice Questions
Biopsy Principles
Practice Questions
Limb Salvage Surgery
Practice Questions
Amputation for Bone Tumors
Practice Questions
Adjuvant Therapies
Practice Questions
Surveillance and Follow-up
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app