
Bone Tumors — MCQs

On this page
Ewing's sarcoma is a PNET (Primitive Neuroectodermal Tumor) that develops in the diaphysis of a long bone. A child with Ewing's sarcoma is on radiotherapy and chemotherapy. Which of the following is a poor prognostic factor in Ewing's sarcoma?
A 28-year-old lady presented with wrist pain. X-ray of the wrist shows a lytic eccentric lesion in the lower end of the radius with a soap bubble appearance. What is the next plan of management?

A 19-year-old male has a small circumscribed sclerotic swelling over the diaphysis of femur, likely diagnosis is:
True about osteoid osteoma is
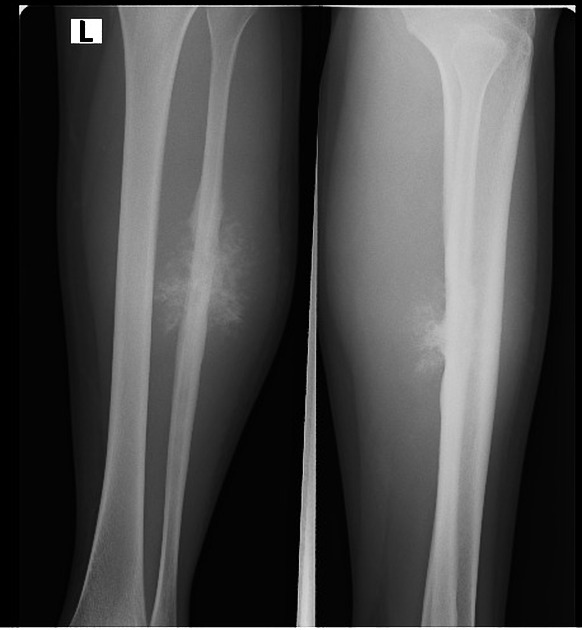
An 8 yr old child is having fever with pain and swelling in mid leg. On Xray lamellated appearance and Codman's triangle is present. Histopathologic examination shows small round cells positive for MIC-2. What is the most likely diagnosis?
True statements about hemangioma of bone: a) Mostly symptomatic b) Peak incidence in 5th decade c) Constitute 1-1.5% of total bone tumors d) Overgrowth of bone occurs
Osteomyelitis can mimic which of the following tumor?
Codman triangle is seen in
Most common site of osteogenic sarcoma is:
A patient with GCT, which of the following is false?
Practice by Chapter
Classification of Bone Tumors
Practice Questions
Benign Bone Tumors
Practice Questions
Malignant Primary Bone Tumors
Practice Questions
Metastatic Bone Disease
Practice Questions
Tumor-Like Lesions of Bone
Practice Questions
Soft Tissue Tumors
Practice Questions
Evaluation and Staging of Bone Tumors
Practice Questions
Biopsy Principles
Practice Questions
Limb Salvage Surgery
Practice Questions
Amputation for Bone Tumors
Practice Questions
Adjuvant Therapies
Practice Questions
Surveillance and Follow-up
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app