
Bone Tumors — MCQs

On this page
All of the following are the causes of sudden increase in pain in osteochondroma, except:
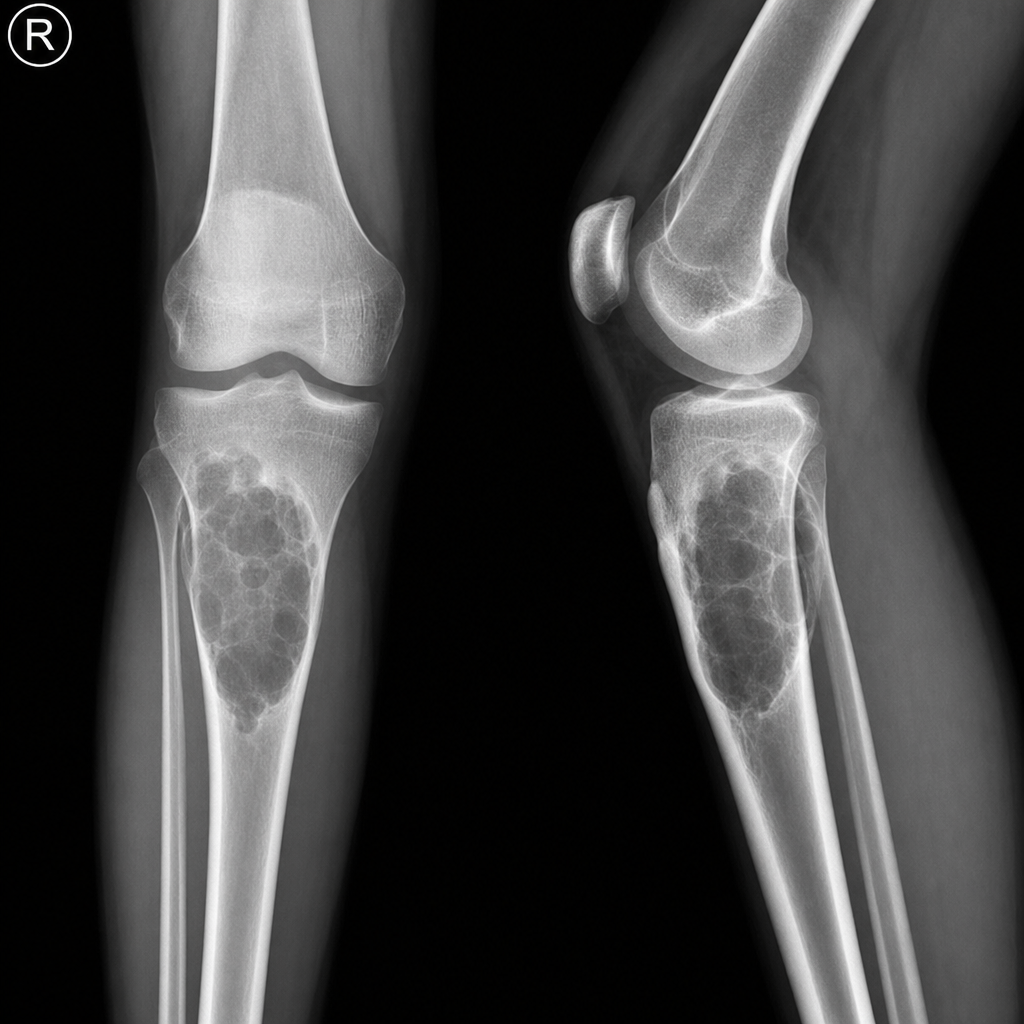
Following X-ray shows the most probable diagnosis as?
Most common benign tumor of bone?
Commonest site of the simple bone cyst is
Most common benign tumor of bone:
Not true about enchondroma
Which of the following is an epiphyseal lesion?
A 45 yrs male presented with an expansile lesion in the centre of femoral metaphysis. The lesion shows Endosteal scalloping and punctuate calcifications. Most likely diagnosis is:
Ewings sarcoma clinically mimics -
Ganga Ram, a 19-year-old male with a short history of pain in the right groin that worsens at night time and has a small circumscribed sclerotic swelling over diaphysis of femur. Likely diagnosis is:
Practice by Chapter
Classification of Bone Tumors
Practice Questions
Benign Bone Tumors
Practice Questions
Malignant Primary Bone Tumors
Practice Questions
Metastatic Bone Disease
Practice Questions
Tumor-Like Lesions of Bone
Practice Questions
Soft Tissue Tumors
Practice Questions
Evaluation and Staging of Bone Tumors
Practice Questions
Biopsy Principles
Practice Questions
Limb Salvage Surgery
Practice Questions
Amputation for Bone Tumors
Practice Questions
Adjuvant Therapies
Practice Questions
Surveillance and Follow-up
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app