
Bone Tumors — MCQs

On this page
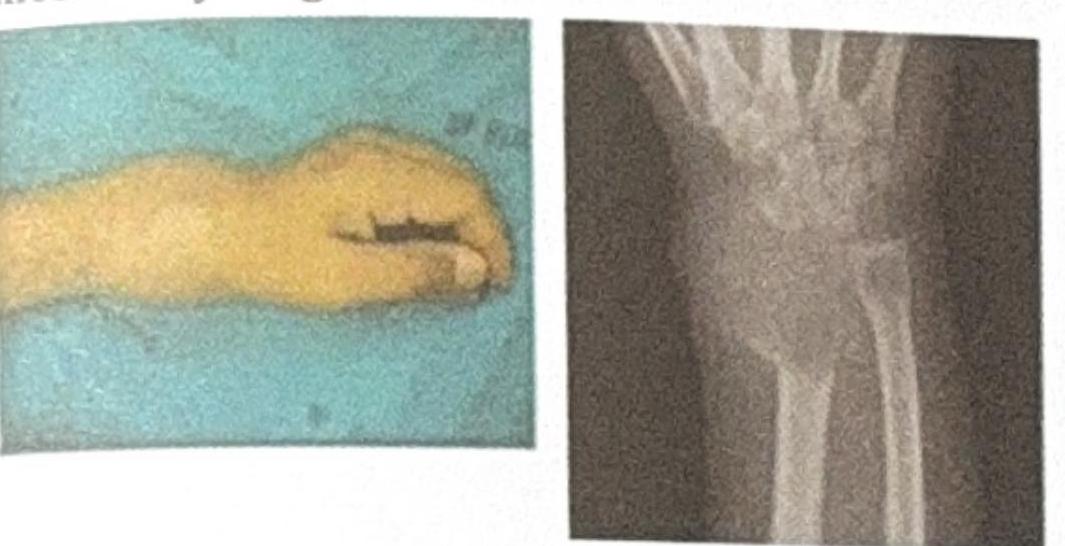
The image shows a wrist deformity and an X-ray of a bone lesion near the distal radius. Based on the clinical and radiological features, what is the most likely diagnosis?
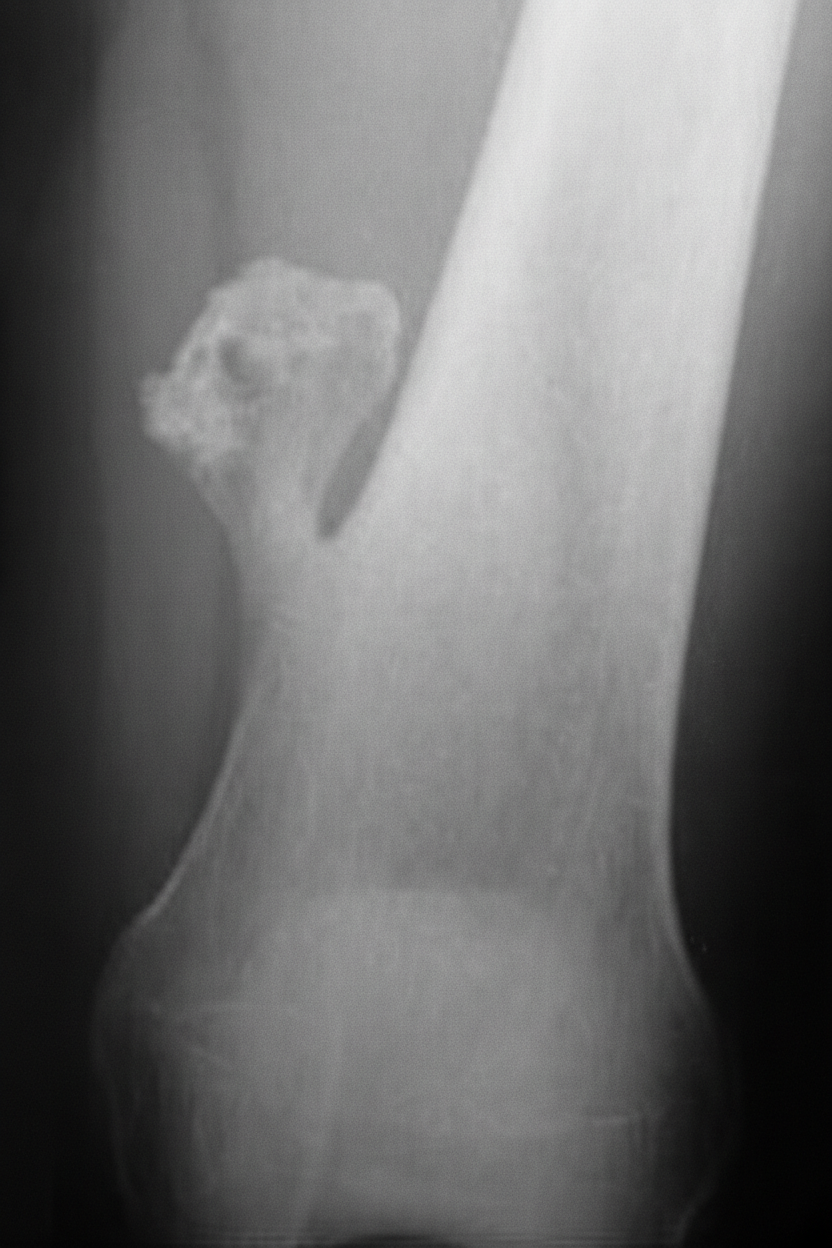
A 14 year old male presents with mushroom like tumor in the distal femur for past 2 years. Which of the following features suggest malignant transformation?
Adamantinoma affects
A patient presents with pain in the thigh, relieved by aspirin. X-ray shows a radiolucent mass surrounded by sclerosis. Diagnosis is ?
Soap bubble appearance on X-ray is seen in which bone tumor?
A 10-year child presented with a mid tibial swelling which an x-ray revealed a lytic lesion with sclerotic margins. What is the most likely diagnosis?

The signs of malignant transformation in osteochondroma are all except
A child 10 yrs of age presents with a mass on his left thigh. The mass seems to be arising from the diaphysis of the femur and involving the soft tissue of the thigh. The child is having fever also. Give your most probable diagnosis -
Classification system of bone tumors is -
A 20-year old male patient presents with pain on movement. X-ray of knee joint shows lytic lesion on the upper end of tibia. What is the likely diagnosis?
Practice by Chapter
Classification of Bone Tumors
Practice Questions
Benign Bone Tumors
Practice Questions
Malignant Primary Bone Tumors
Practice Questions
Metastatic Bone Disease
Practice Questions
Tumor-Like Lesions of Bone
Practice Questions
Soft Tissue Tumors
Practice Questions
Evaluation and Staging of Bone Tumors
Practice Questions
Biopsy Principles
Practice Questions
Limb Salvage Surgery
Practice Questions
Amputation for Bone Tumors
Practice Questions
Adjuvant Therapies
Practice Questions
Surveillance and Follow-up
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app