
Bone Tumors — MCQs

On this page
97. Spot the diagnosis based on X-ray:

A 15-year-old boy presents with pain in the right upper arm and stiffness after playing cricket in the school. Since the complaints of the child were persisting, the family physician performed X-ray of right upper arm. The X-ray humerus shows presence of:

Spot the diagnosis based on the given X-ray of hand.

Comment on the diagnosis of the presentation shown below:

All are correct about the condition shown in X-ray except:

A skeletally mature adult presents with the following X-ray. Identify the lesion shown below:

The most likely diagnosis for the lesion shown in the image is:

The following hallmarks characterise Diaphyseal aclasis except
The most common site for osteosarcoma is:
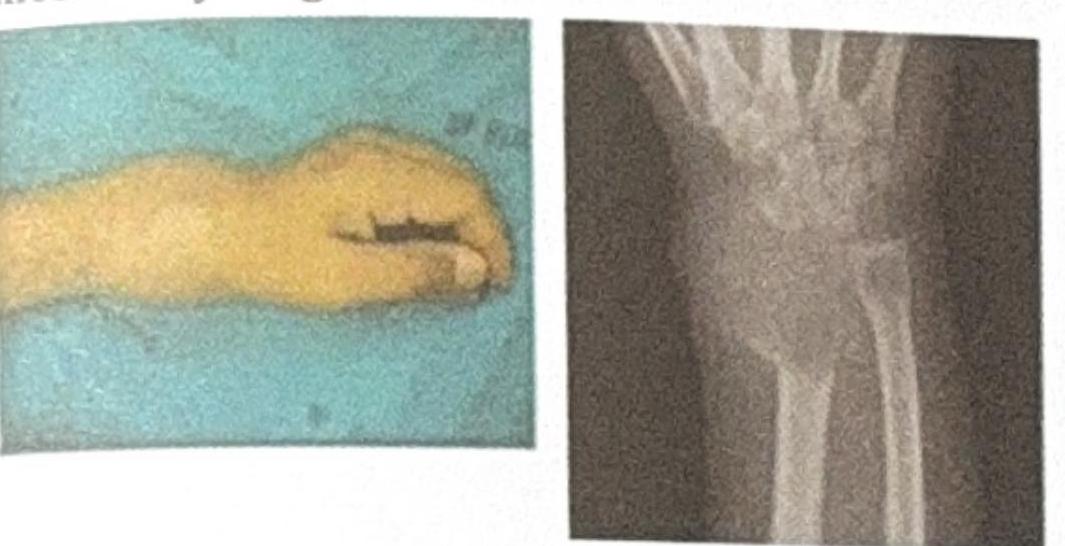
The image shows a wrist deformity and an X-ray of a bone lesion near the distal radius. Based on the clinical and radiological features, what is the most likely diagnosis?
Practice by Chapter
Classification of Bone Tumors
Practice Questions
Benign Bone Tumors
Practice Questions
Malignant Primary Bone Tumors
Practice Questions
Metastatic Bone Disease
Practice Questions
Tumor-Like Lesions of Bone
Practice Questions
Soft Tissue Tumors
Practice Questions
Evaluation and Staging of Bone Tumors
Practice Questions
Biopsy Principles
Practice Questions
Limb Salvage Surgery
Practice Questions
Amputation for Bone Tumors
Practice Questions
Adjuvant Therapies
Practice Questions
Surveillance and Follow-up
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app