
Bone Tumors — MCQs

On this page
An eight-year-old boy presents with back pain and mild fever. His plain X-ray of the dorsolumbar spine reveals a solitary collapsed dorsal vertebra with preserved disc spaces. There was no associated soft tissue shadow. What is the most likely diagnosis?
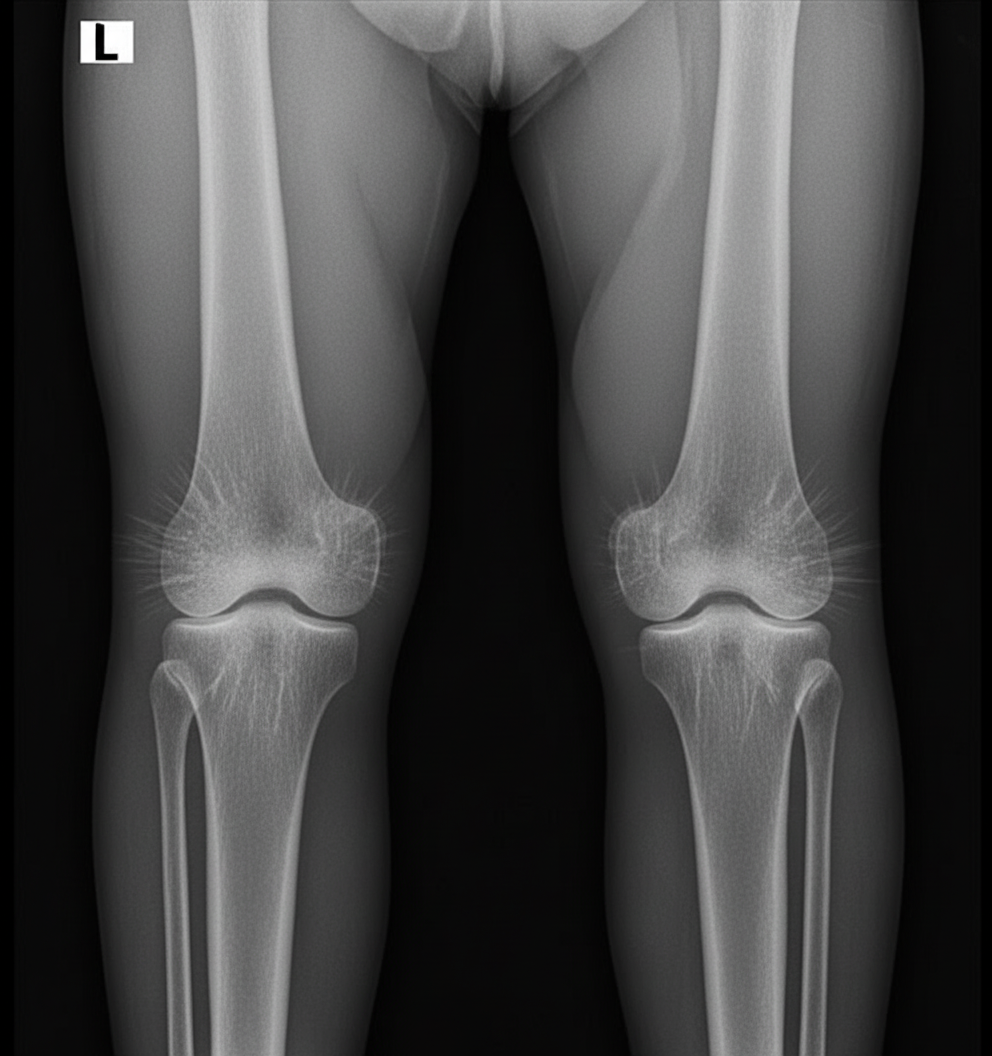
An 11-year-old boy presents with pain in his right leg. A radiograph shows a "sunburst" appearance with bone destruction, soft tissue mass, new bone formation, and sclerosis limited to the metaphysis of the lower femur. Select the type of bone lesion with which it is most likely to be associated.
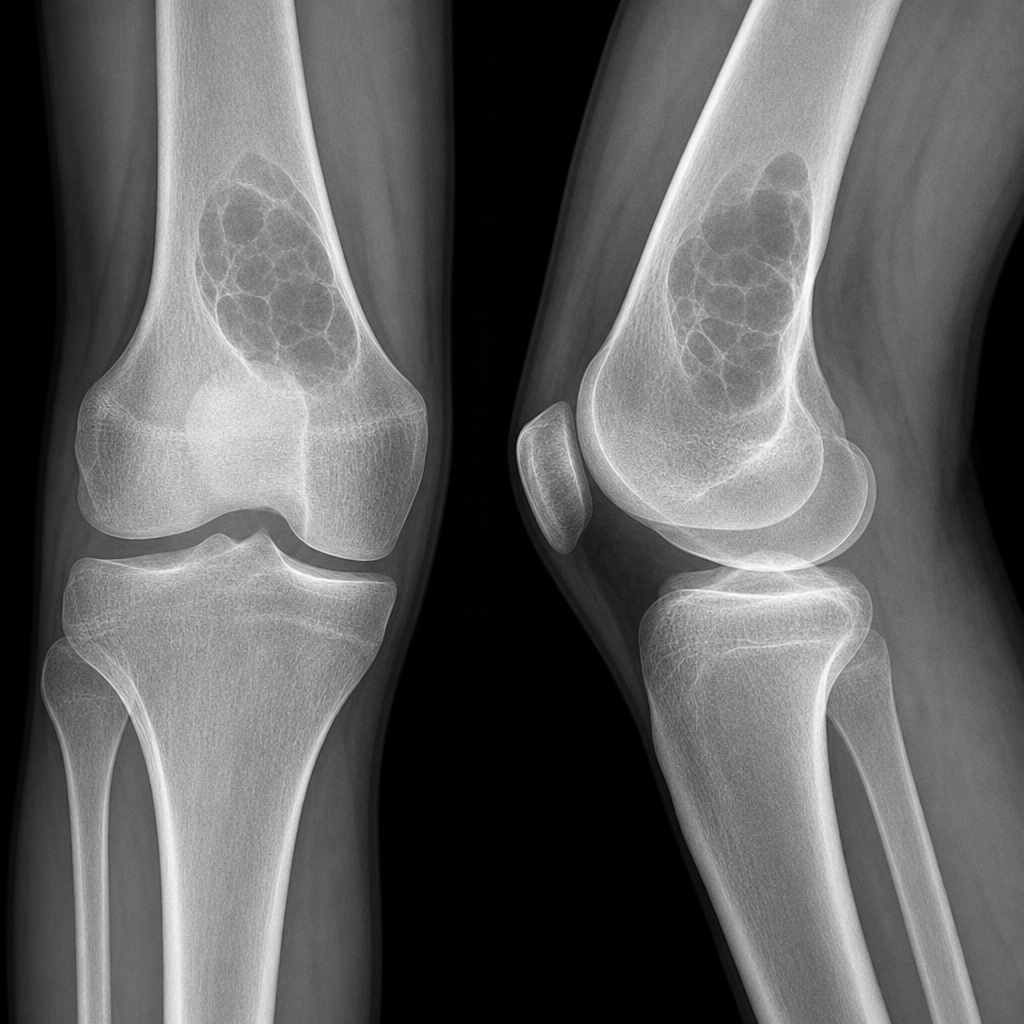
The X-ray of a knee in an adolescent boy is shown. What is the probable diagnosis?
What is the typical time period between the occurrence of osteosarcoma following radiation therapy?
What is the most common tumor of the vertebral spine in adults?
Which of the following conditions is characterized by a "moth-eaten" bone appearance?
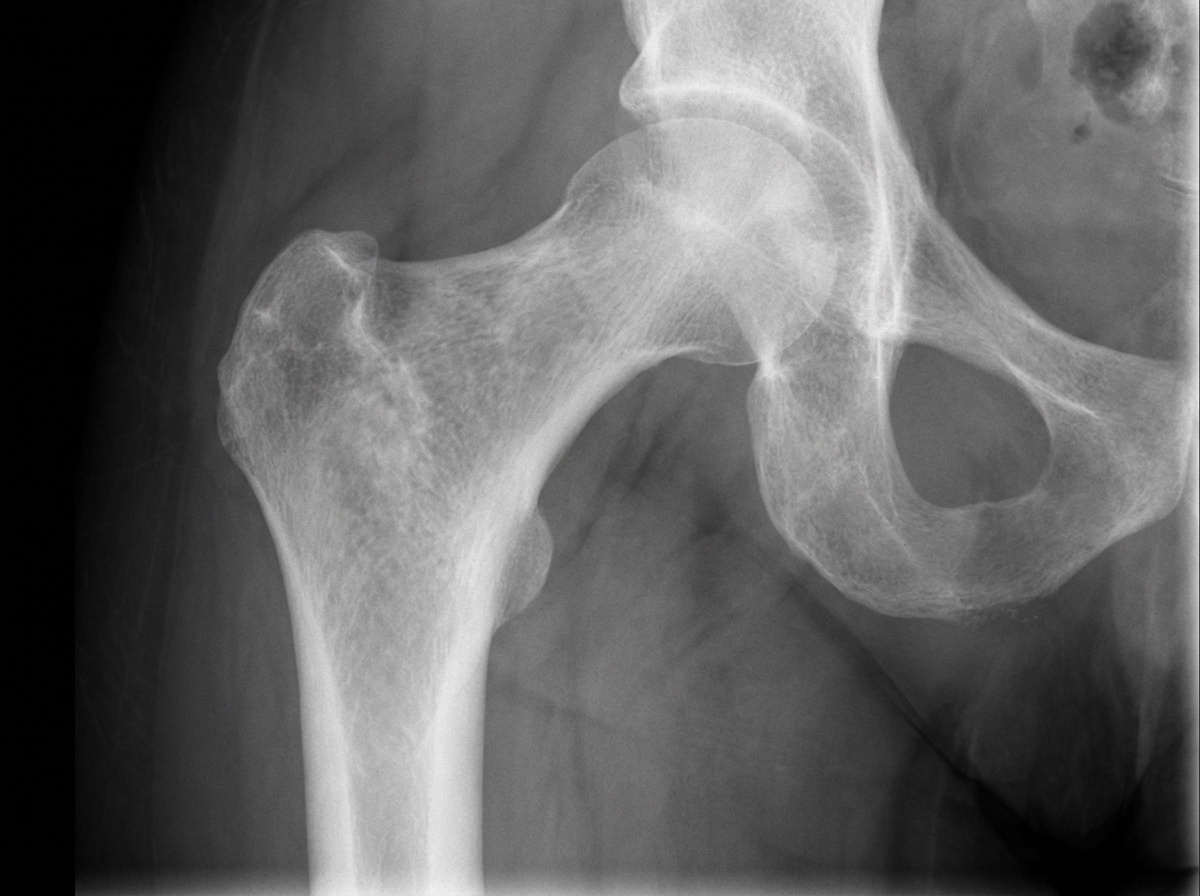
An X-ray of the proximal femur in a patient presenting with hip pain shows a specific deformity. What is this deformity?
Which of the following is NOT a common site of primary bone metastasis?
All of the following statements regarding Ewing's sarcoma are true EXCEPT?
What is the most probable diagnosis based on the X-ray findings in a 20-year-old female presenting with knee swelling?
Practice by Chapter
Classification of Bone Tumors
Practice Questions
Benign Bone Tumors
Practice Questions
Malignant Primary Bone Tumors
Practice Questions
Metastatic Bone Disease
Practice Questions
Tumor-Like Lesions of Bone
Practice Questions
Soft Tissue Tumors
Practice Questions
Evaluation and Staging of Bone Tumors
Practice Questions
Biopsy Principles
Practice Questions
Limb Salvage Surgery
Practice Questions
Amputation for Bone Tumors
Practice Questions
Adjuvant Therapies
Practice Questions
Surveillance and Follow-up
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app