
Bone Grafts and Substitutes — MCQs

On this page
Which site is the most common source for autologous bone grafts?
Clamshell technique is required for which type of bone graft?
Cancellous bone graft can be taken from which of the following anatomical locations?
Which of the following bone grafts possesses osteogenic properties?
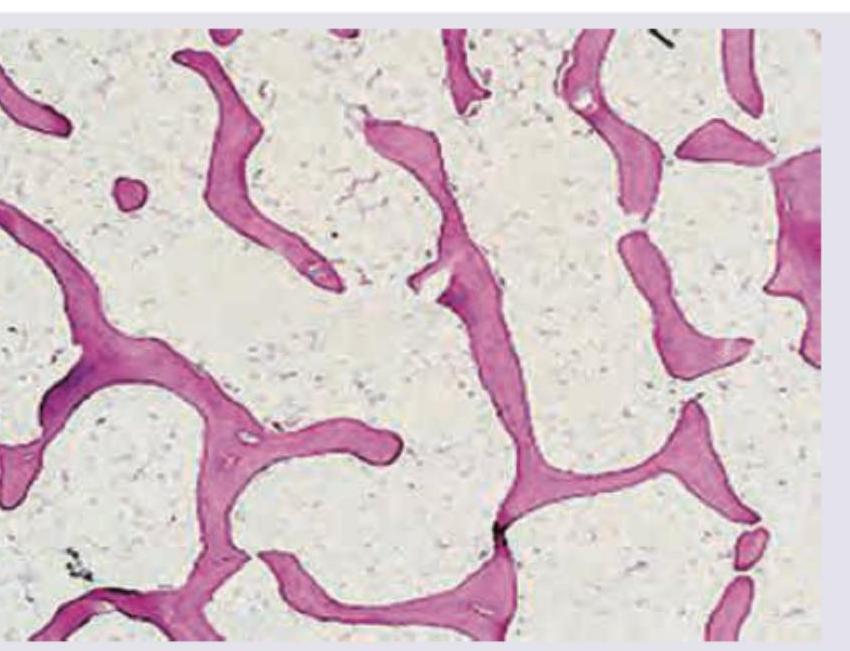
All are correct about the bone tissue shown except:
Which of the following bone defects offers the best chance for bone fill?
The graft with the maximum osteogenic potential is:
Which of the following statements are correct about Kiel bone? 1. Xenograft 2. Allograft 3. Treated by detergent, sterilized, and freeze-dried 4. Ox or calf bone denatured with 20% H2O2, acetone, and sterilized
Which of the following has the greatest concentration of osteogenic cells?
Practice by Chapter
Biology of Bone Grafting
Practice Questions
Autografts: Harvesting and Applications
Practice Questions
Allografts: Processing and Applications
Practice Questions
Bone Graft Substitutes
Practice Questions
Vascularized Bone Grafts
Practice Questions
Growth Factors in Bone Healing
Practice Questions
Demineralized Bone Matrix
Practice Questions
Ceramic Materials
Practice Questions
Composite Grafts
Practice Questions
Bone Graft Immunology
Practice Questions
Bone Morphogenetic Proteins
Practice Questions
Tissue Engineering in Orthopaedics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app