
Basic Science in Orthopaedics — MCQs

On this page
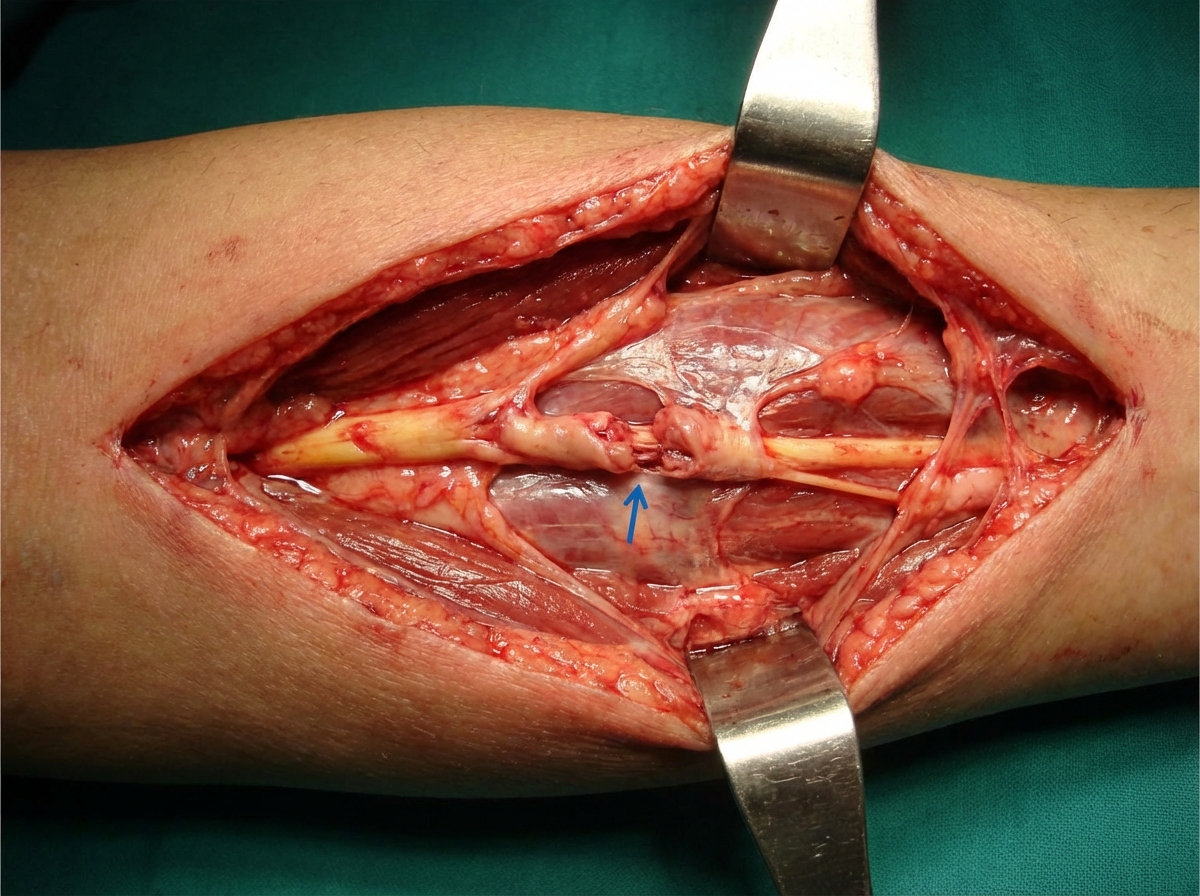
A 50-year-old male presented to the orthopedic OPD for regular follow-up, being treated for a forearm injury marked in a specimen. During examination, the doctor elicited a specific sign by tapping over the advancing regeneration front of the nerve, causing the patient to feel a tingling sensation in its distal distribution. What is the rate of peripheral axonal regeneration from the proximal stump?
In achondroplasia, a mutation occurs in which of the following genes?
Which of the following is not a good prognostic indicator?
Osteonecrosis is not seen in which of the following conditions?
The tensile strength of a bone is due to which component?
Which subtype of Osteogenesis imperfecta is not associated with blue sclera?
The basic pathology in Myositis Ossificans Progressiva is located in which of the following?
A patient develops Saturday Night Palsy after consuming alcohol and sleeping overnight with an arm in a dependent position. Which of the following best describes the clinical manifestations of this condition?
Which of the following factors does NOT facilitate non-union of a fracture?
What is the major mineral component of bone?
Practice by Chapter
Bone Structure and Function
Practice Questions
Cartilage Biology and Physiology
Practice Questions
Muscle and Tendon Physiology
Practice Questions
Joint Biomechanics
Practice Questions
Fracture Healing Process
Practice Questions
Bone Metabolism and Turnover
Practice Questions
Orthopaedic Biomaterials
Practice Questions
Tribology in Orthopaedics
Practice Questions
Gait Analysis
Practice Questions
Biomechanics of Spine
Practice Questions
Applied Surgical Anatomy
Practice Questions
Bone Banking and Grafting
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app