
Tuberculosis of Bones and Joints — MCQs

A healthcare worker develops fever, night sweats, and cough. Sputum shows acid-fast bacilli. What is the next diagnostic test?
According to DOTS-PLUS guidelines 2013, which of the following statements about the treatment of multidrug-resistant TB is incorrect?
A patient with pulmonary tuberculosis, who is receiving anti-tuberculosis therapy consisting of rifampicin, isoniazid, ethambutol, and pyrazinamide, should be advised to take which of the following supplements?
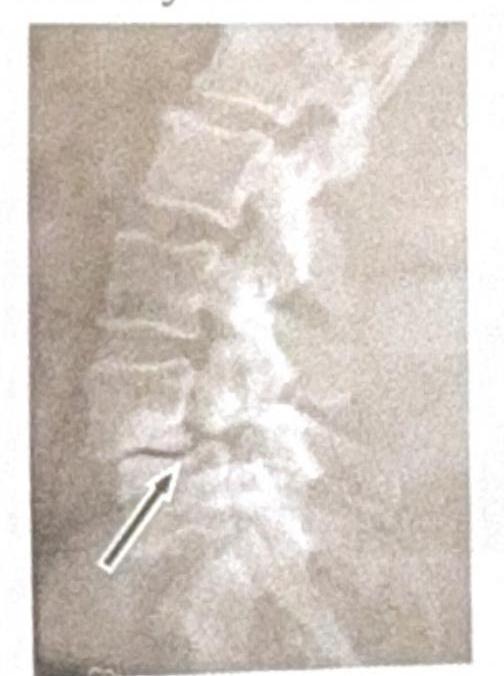
Identify the condition shown in the image:
In tuberculosis, a 'case' is
A 60-year-old male presents with chronic arthritis. Which of the following is the most likely cause?
A 75-year-old female has chronic backache. X-ray of the spine is shown. What is the most likely diagnosis?

What is considered a poor prognostic indicator in Pott's paraplegia?
Tuberculosis of the spine; what is the most common site affected?
What is the earliest X-ray sign observed in spinal tuberculosis?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app