
LASIK — MCQs

10 questions
Read Study NotesQ1
Which laser is used in the management of posterior capsule opacification (PCO)?
Q2
Which of the following is not a relative contraindication for breast conservative surgery?
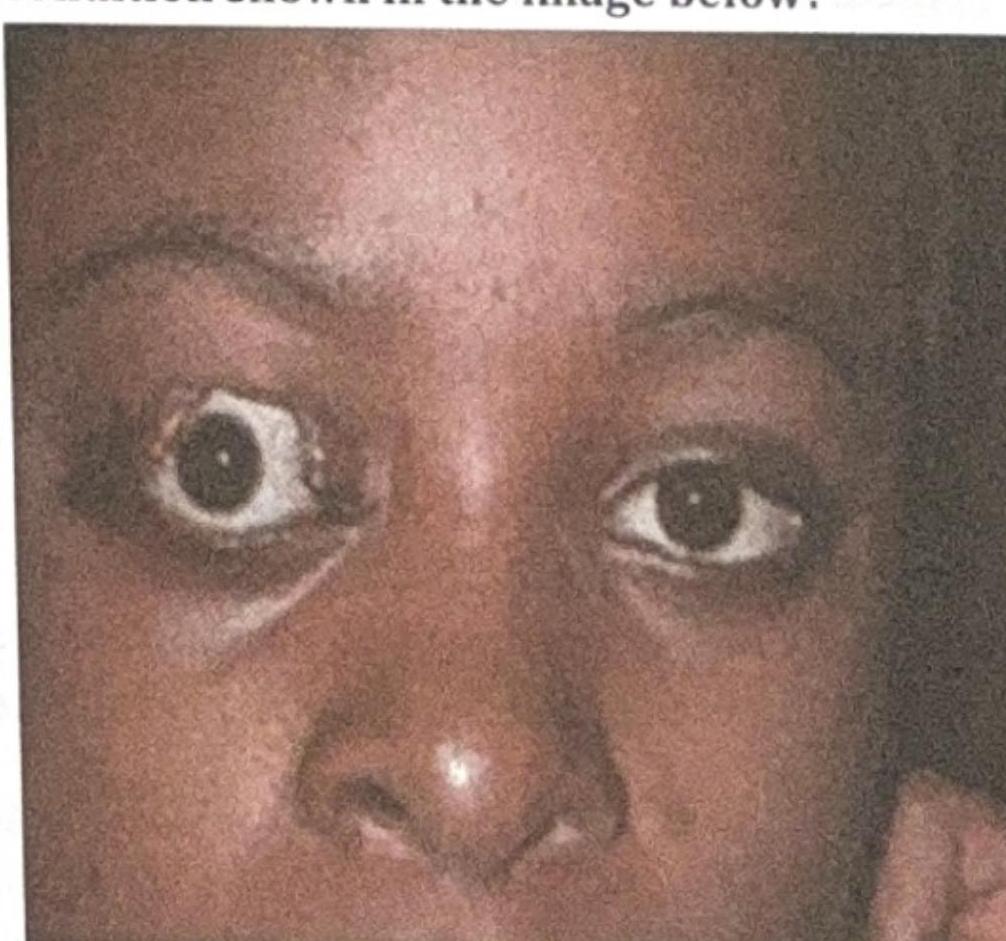
Q3
What is the most likely complication of the condition shown in the image below?
Q4
Which keratometry reading is most accurate in post-LASIK eyes for IOL power calculation?
Q5
Laser used in LASIK is:
Q6
The laser procedure, most often used for treating iris neovascularization is
Q7
Maximum correction of myopia can be done by?
Q8
What does a visual acuity test primarily assess?
Q9
Which of the following is a contraindication to topical steroids?
Q10
Absolute contraindication for LASIK is:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app