
Pediatric Ophthalmology and Strabismus — MCQs

On this page
Amplitude of accommodative convergence is:
Spontaneous absorption of lenticular material and bilateral microphthalmos is seen in which of the following conditions?
Deviation of near vision is conveniently tested by?
All of the following are employed to evaluate a case of heterophoria except?
Secondary deviation of the eye is an example of which of the following laws?
Brown's syndrome involves dysfunction of which muscle?
Miotics are used in which type of squint?
Esotropia is associated with which of the following refractive errors?
Which of the following is NOT a manifestation of squint in children?
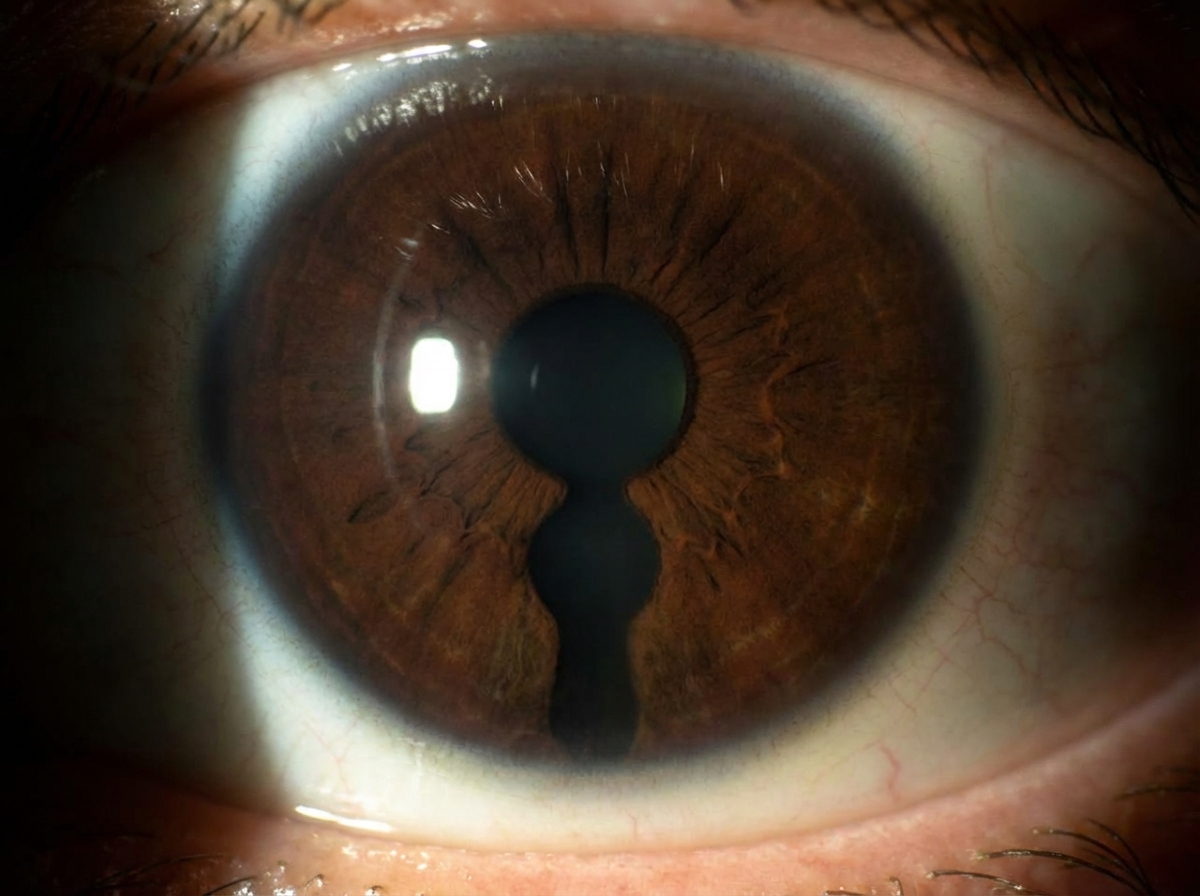
What term is used to describe the finding?
Practice by Chapter
Amblyopia
Practice Questions
Esotropia
Practice Questions
Exotropia
Practice Questions
Vertical Deviations
Practice Questions
Special Forms of Strabismus
Practice Questions
Nystagmus in Children
Practice Questions
Pediatric Cataract
Practice Questions
Retinopathy of Prematurity
Practice Questions
Pediatric Glaucoma
Practice Questions
Pediatric Neuro-ophthalmology
Practice Questions
Genetic Eye Diseases in Children
Practice Questions
Pediatric Ocular Trauma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app