
Pediatric Ophthalmology and Strabismus — MCQs

On this page
The cover-uncover test is performed to diagnose various eye conditions. Which of the following is not detected by this test?
A 5-month-old baby is brought by the mother with complaints of the left upper eyelid moving up and down during breastfeeding or thumb sucking, which disappears when the baby is not being fed. What is the most likely diagnosis?
A 3-year-old child has amblyopia in the right eye. What is the preferred treatment for this child?
All of the following are done in the treatment of amblyopia, except:
The essential foundational components of binocular single vision are:
Identify the clinical sign shown in the picture:

Based on the clinical photograph, identify the type of strabismus present:

All are causes of the presentation shown below except:
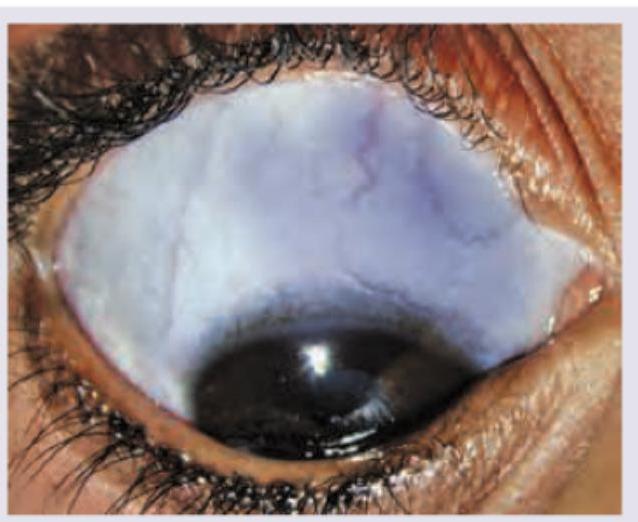
A 6-month-old child with retinoblastoma is brought with the following presentation in the right eye. The presentation shown is known as:
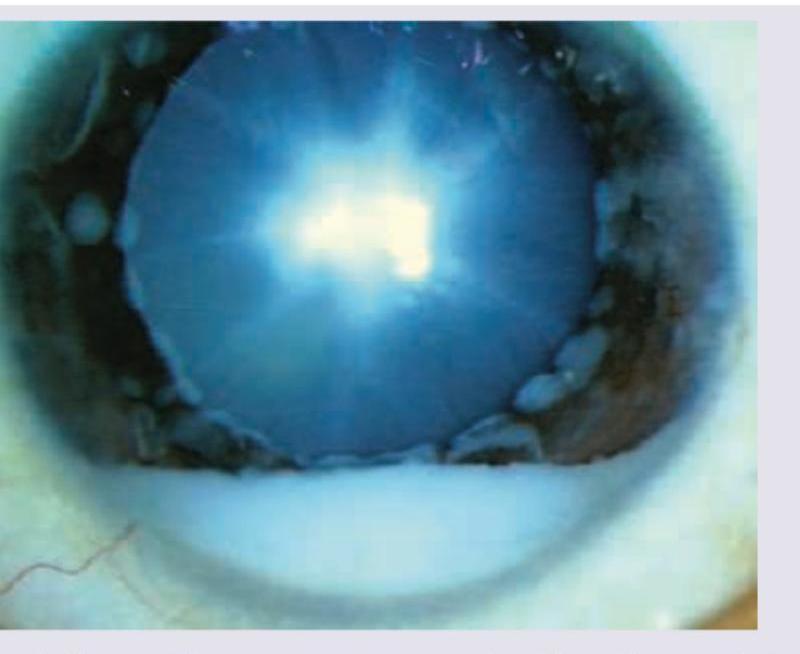
A 2-year-old child is brought with complaints of watering of eyes, photophobia and intermittently keeping eyes closed while watching TV. What may be the diagnosis? (AIIMS Nov 2018)

Practice by Chapter
Amblyopia
Practice Questions
Esotropia
Practice Questions
Exotropia
Practice Questions
Vertical Deviations
Practice Questions
Special Forms of Strabismus
Practice Questions
Nystagmus in Children
Practice Questions
Pediatric Cataract
Practice Questions
Retinopathy of Prematurity
Practice Questions
Pediatric Glaucoma
Practice Questions
Pediatric Neuro-ophthalmology
Practice Questions
Genetic Eye Diseases in Children
Practice Questions
Pediatric Ocular Trauma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app