
Orbital Diseases — MCQs

On this page
Which of the following is NOT a cause of pseudo-proptosis?
Which childhood malignancy commonly presents with proptosis?
What is the commonest histological type of rhabdomyosarcoma of the orbit?
Thyroid ophthalmopathy is associated with all of the following except:
A child presents with unilateral proptosis which is compressible and increases on bending forwards. It is non-pulsatile and has no thrill or bruit. MRI shows retroorbital mass with echogenic shadows. What is the most probable diagnosis?
A blowout fracture of the orbit refers to which of the following?
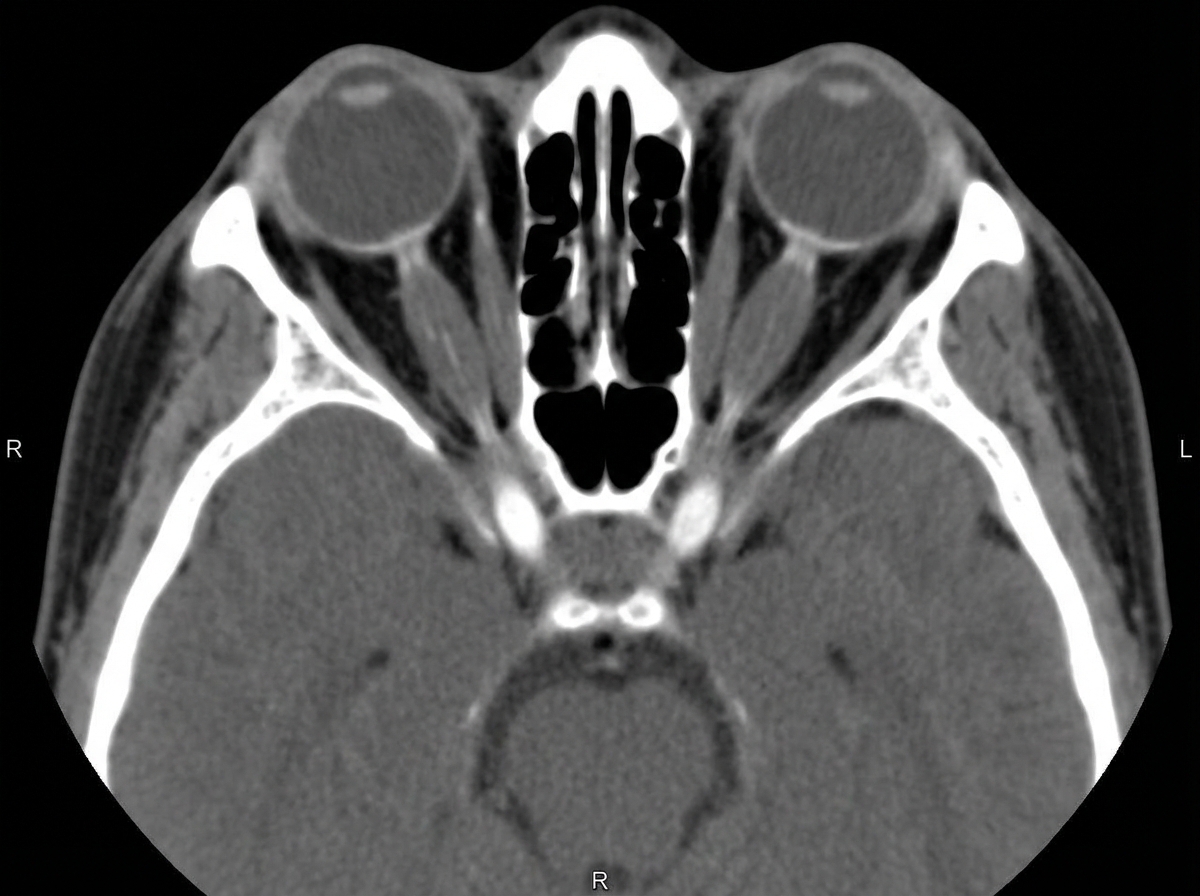
What is the cause for enlargement of the extraocular muscles shown in this CT-scan?
A 8-year-old boy presented with a 3-month history of left eye swelling. Examination revealed left eye proptosis with preserved vision. The right eye is normal. A CT scan revealed an intraorbital extraconal mass lesion. Biopsy revealed embryonal rhabdomyosarcoma. Metastatic workup was normal. What is the standard line of treatment?
Which of the following is characteristic of dysthyroid eye disease of Type-1 orbitopathy?
What is the most common cause of orbital cellulitis?
Practice by Chapter
Orbital Anatomy
Practice Questions
Orbital Imaging Techniques
Practice Questions
Orbital Inflammations
Practice Questions
Orbital Infections
Practice Questions
Orbital Tumors: Primary
Practice Questions
Orbital Tumors: Secondary
Practice Questions
Vascular Lesions of Orbit
Practice Questions
Thyroid Orbitopathy
Practice Questions
Orbital Trauma
Practice Questions
Congenital Orbital Anomalies
Practice Questions
Orbital Surgery Techniques
Practice Questions
Enucleation and Exenteration
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app