
Orbital Diseases — MCQs

On this page
Axial proptosis is produced by tumors lying in:
Most common malignant intraorbital tumor in adults is?
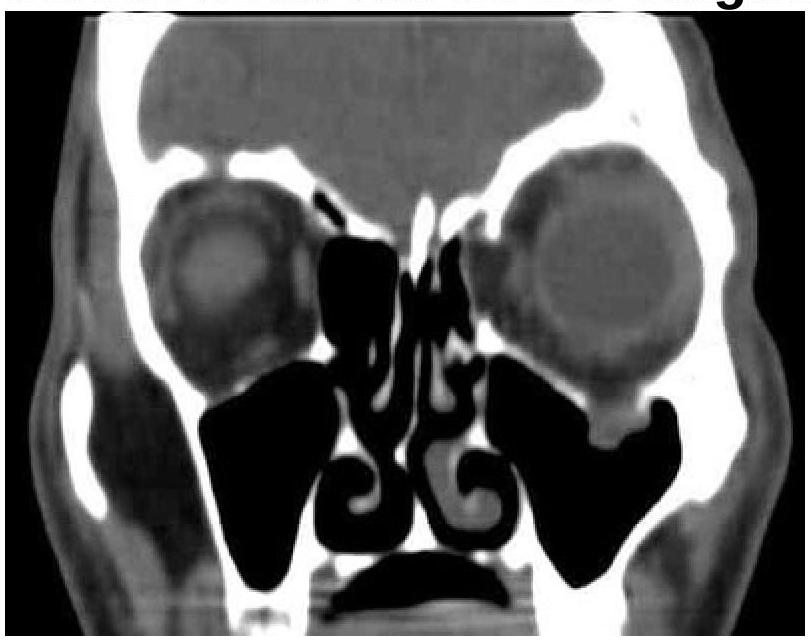
A patient presented with a history of diplopia and restricted eye movements. What is the most likely diagnosis based on the clinical and CT images?
Blowout fracture of the orbit most commonly involves?
Which of the following conditions is least likely to cause proptosis?
What is the most common orbital tumor in children?
What is the most common cause of intermittent proptosis in adults?
Which muscle is the earliest to be involved in thyroid ophthalmopathy?
Most common orbital tumor has its origin from?
The muscle first affected in thyroid ophthalmopathy is:
Practice by Chapter
Orbital Anatomy
Practice Questions
Orbital Imaging Techniques
Practice Questions
Orbital Inflammations
Practice Questions
Orbital Infections
Practice Questions
Orbital Tumors: Primary
Practice Questions
Orbital Tumors: Secondary
Practice Questions
Vascular Lesions of Orbit
Practice Questions
Thyroid Orbitopathy
Practice Questions
Orbital Trauma
Practice Questions
Congenital Orbital Anomalies
Practice Questions
Orbital Surgery Techniques
Practice Questions
Enucleation and Exenteration
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app