
Orbital Diseases — MCQs

On this page
Which of the following statements about Orbital Rhabdomyosarcoma is incorrect?
Which of the following tumors presents with proptosis?
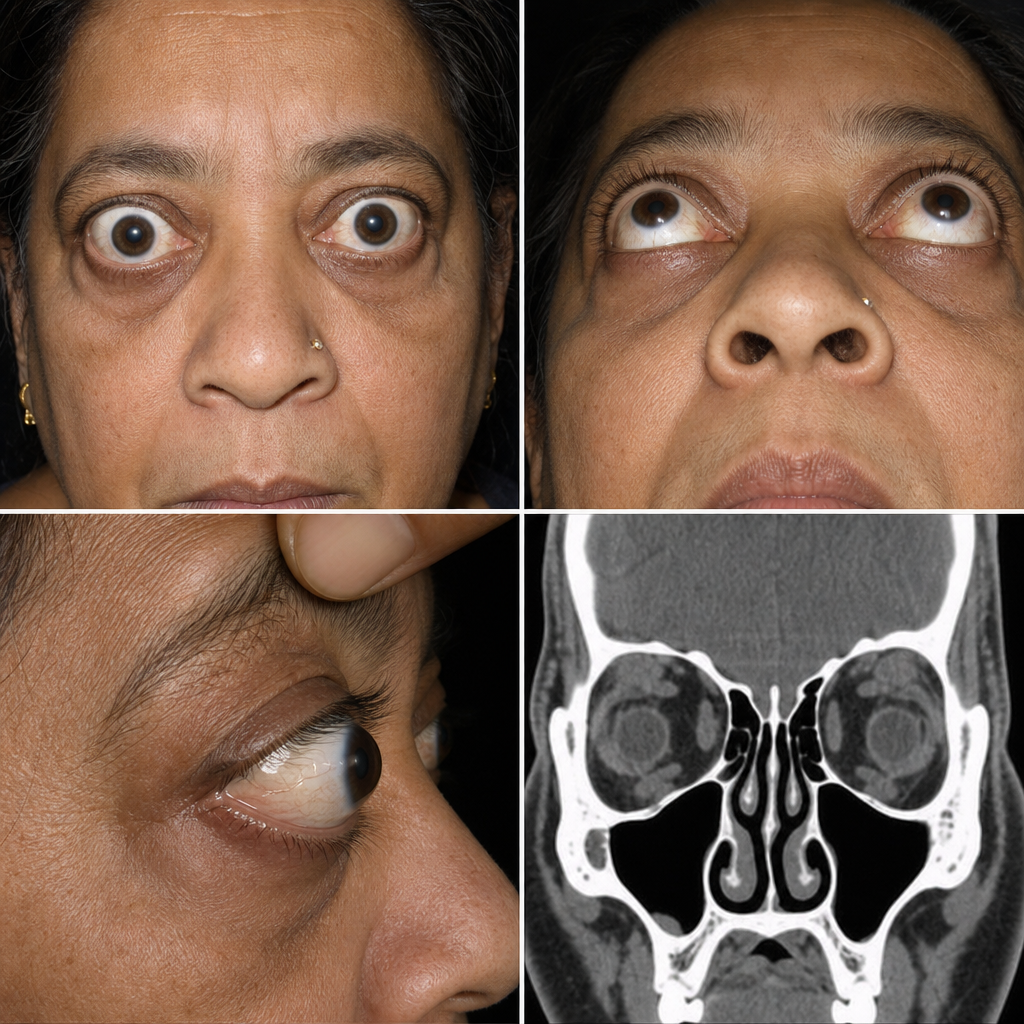
What is the most common cause of unilateral proptosis?
A patient presents with proptosis that increases when bending down. What is the most likely diagnosis?
Which of the following is true about orbital cellulitis?
A 15-year-old female presents with a painless, gradually increasing mass located at the superotemporal orbital rim (upper outer quadrant of the orbit), present for the past 10 years. On examination, the mass is non-tender and slowly progressive. What is the most likely diagnosis?
A 25-year-old lady presents with development of proptosis on Valsalva maneuver. Diagnosis is:
A 3-year-old girl brought with swelling in left eye which had shown rapid growth in last 4 weeks. On examination it is a bulbous fleshy mass about 5 x 4 cm arising from lower eyelid. No organomegaly or was noted and lymph node examination was unremarkable. The Complete blood counts are normal. Probable diagnosis is?
Which of the following statements is false? 
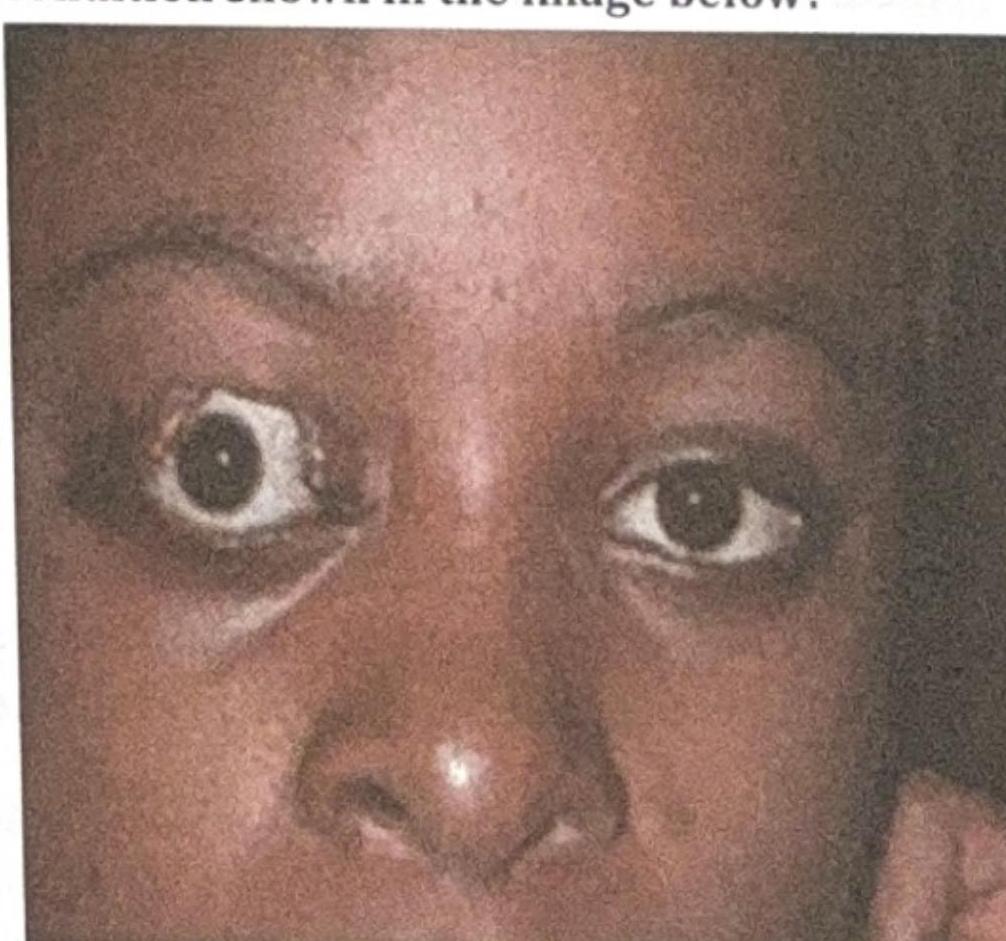
What is the most likely complication of the condition shown in the image below?
Practice by Chapter
Orbital Anatomy
Practice Questions
Orbital Imaging Techniques
Practice Questions
Orbital Inflammations
Practice Questions
Orbital Infections
Practice Questions
Orbital Tumors: Primary
Practice Questions
Orbital Tumors: Secondary
Practice Questions
Vascular Lesions of Orbit
Practice Questions
Thyroid Orbitopathy
Practice Questions
Orbital Trauma
Practice Questions
Congenital Orbital Anomalies
Practice Questions
Orbital Surgery Techniques
Practice Questions
Enucleation and Exenteration
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app