
Visual Acuity and Contrast Sensitivity — MCQs

Which of the following is the first visual field defect in open-angle glaucoma?
A patient complains of an inability to read a newspaper, particularly in bright sunlight. What is the most likely diagnosis?
According to WHO ICD-11 classification, visual impairment in the better eye (with best correction) begins at a visual acuity worse than:
A 12-year-old boy is admitted to the emergency department with signs of meningitis. To determine the specific type of meningitis, it is necessary to aspirate cerebrospinal fluid with a lumbar puncture for laboratory examination. However, before performing a lumbar puncture, it must be established that the cerebrospinal fluid pressure is not elevated. What condition in the eye would indicate that cerebrospinal fluid pressure is too elevated for a lumbar puncture to be performed?
Under Vision 2020, to check visual acuity, a teacher will refer a school child to
Which of the following best predicts the need for lumbar puncture in a patient with syphilis?
Maximum correction of myopia can be done by?
1mm change in axial length of the eyeball would change the refracting power of the eye by?
A person with a visual acuity of 6/60 in the right eye and 3/60 in the left eye would be categorized into which type of blindness?
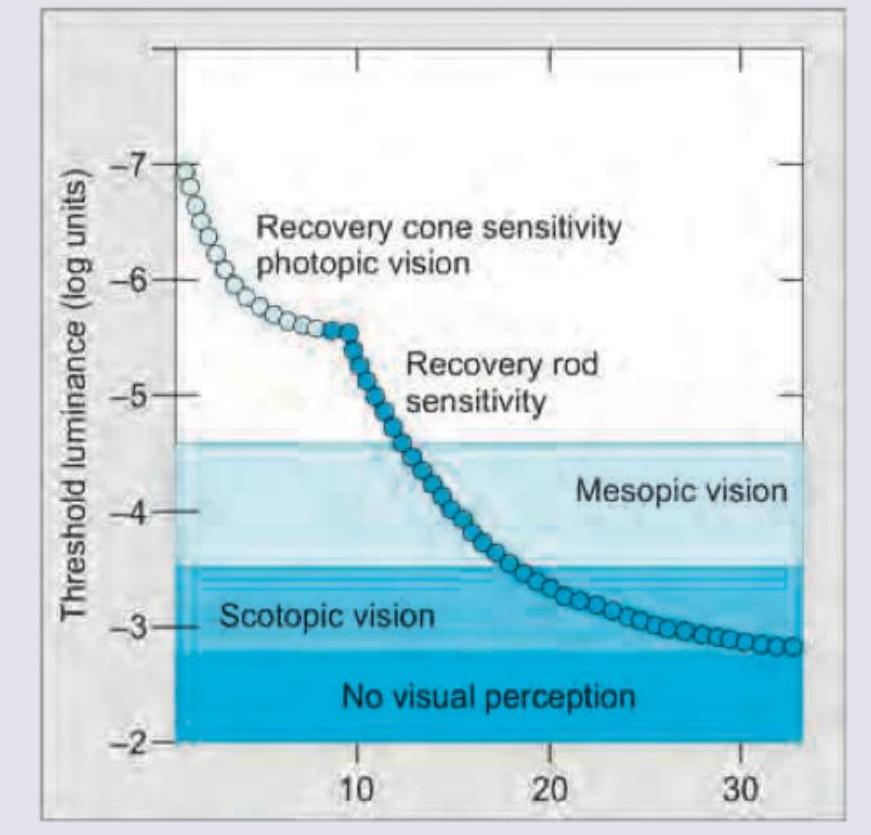
The image given below shows:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app