
Optics and Refraction — MCQs

On this page
What is the true statement about retinoscopy with a plane mirror?
Keratometer is used to assess:
The eye in the newborn is:
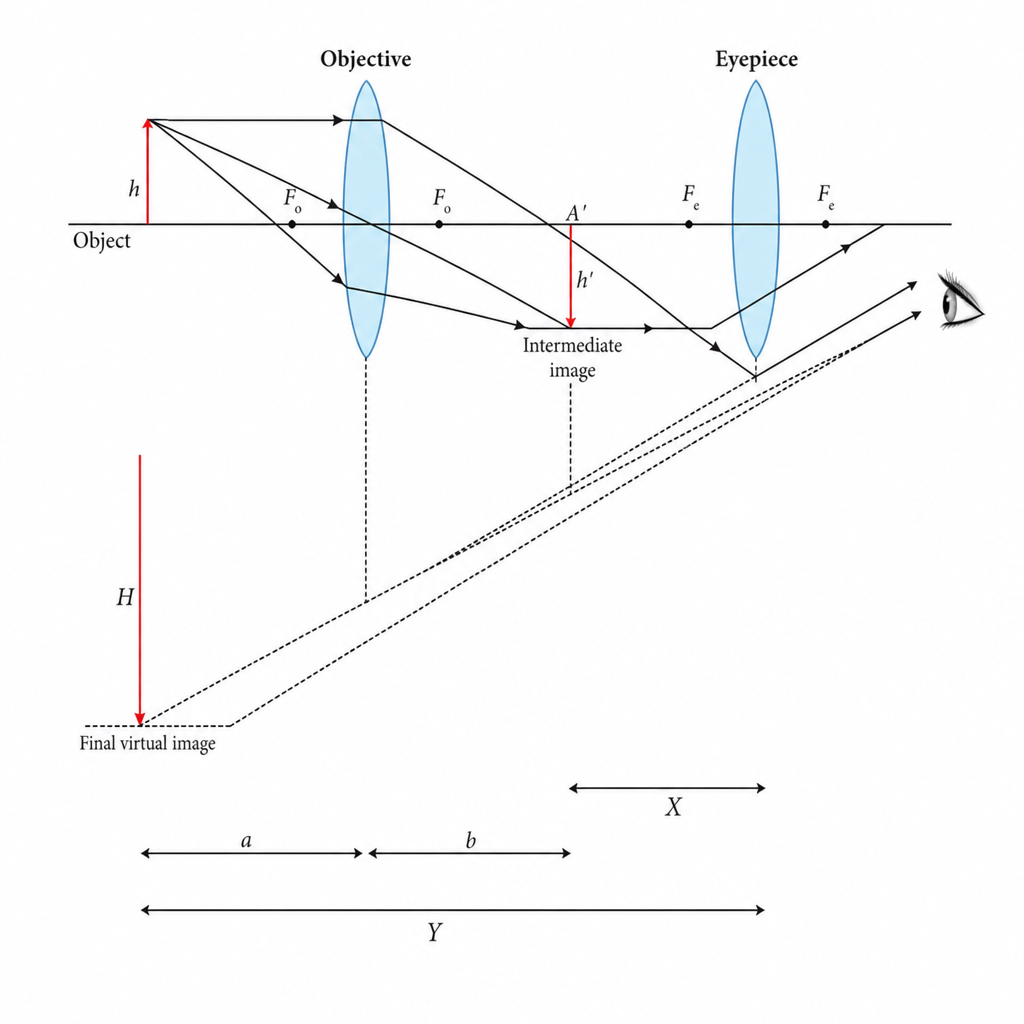
Derive the objective magnification from the following illustration:
Which of the following is a true statement regarding the human eye?
A 50-year-old patient has difficulty reading close objects. Likely diagnosis?
What is anisometropia?
Which structure of the eye is responsible for adjusting focus to clearly view objects at varying distances?
What is the typical magnitude of against-the-rule astigmatism that develops in an elderly patient with a previously emmetropic eye?
Which is an example of Simple Myopic Astigmatism?
Practice by Chapter
Physical Optics
Practice Questions
Geometric Optics
Practice Questions
Optical System of Eye
Practice Questions
Visual Acuity and Contrast Sensitivity
Practice Questions
Refractive Errors
Practice Questions
Accommodation and Presbyopia
Practice Questions
Optical Instruments
Practice Questions
Lenses and Prisms
Practice Questions
Retinoscopy
Practice Questions
Subjective Refraction
Practice Questions
Contact Lens Optics
Practice Questions
Wavefront Technology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app