
Optics and Refraction — MCQs

On this page
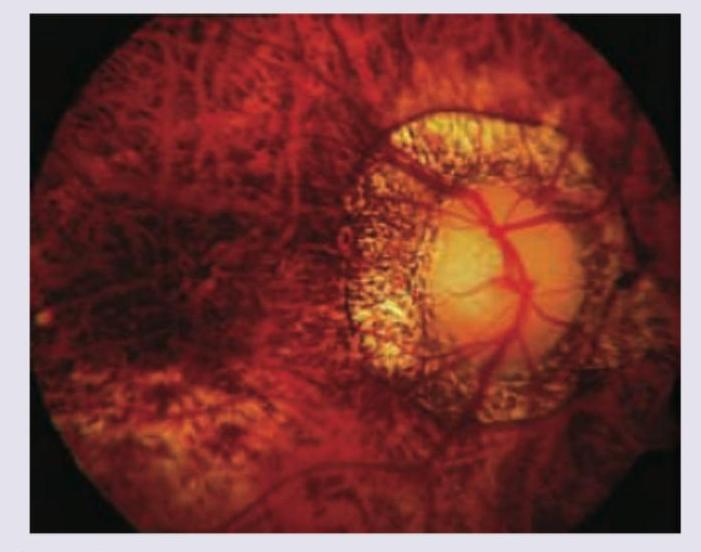
What does the given image show?

All are true about the condition shown in the fundus finding except: (Recent NEET Pattern 2016-17)
The chart shown in the image is:
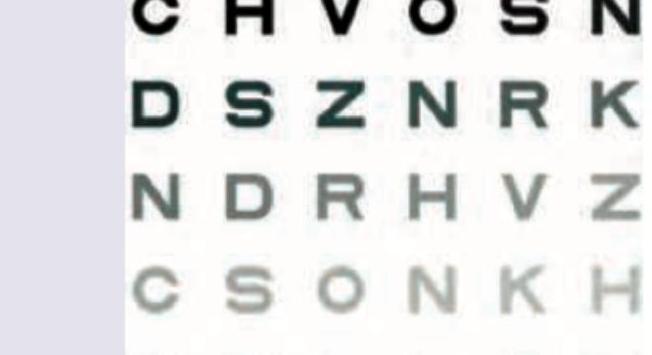
The following 6/6 optotype of Snellen's chart, viewed at 6 meters, will subtend an angle of how many minutes at nodal point of the eye?

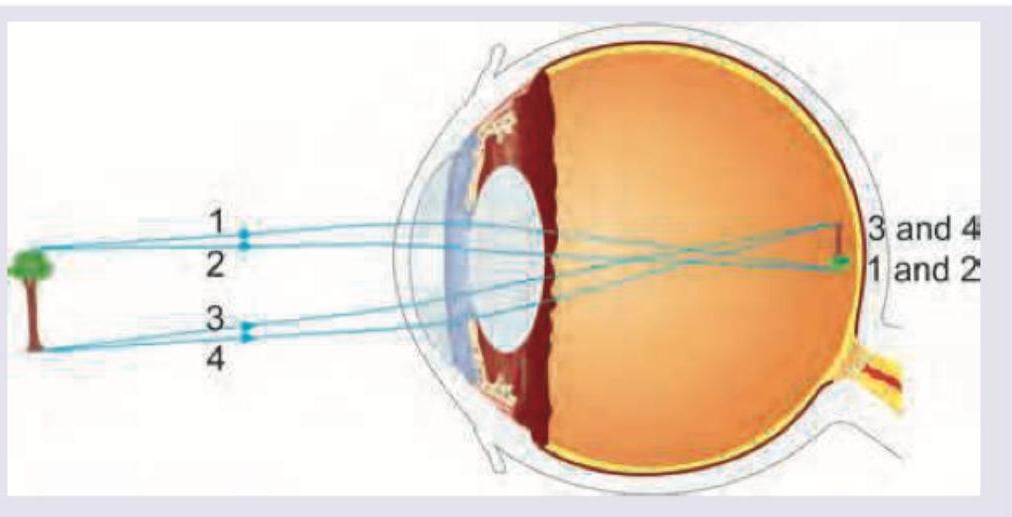
Identify the refractive error shown in the image:
A 52-year-old patient presents with difficulty reading fine print and near work, with gradual onset over the past few years. The following spectacle (Add power: +2.00 D) is prescribed for this patient. What is the primary indication? (AIIMS Nov 2018)

What is the SI unit of illuminance (brightness of light on a surface)?
Average hypermetropia in a newborn is
Campimetry is used to measure:
Keratometry is done to assess:
Practice by Chapter
Physical Optics
Practice Questions
Geometric Optics
Practice Questions
Optical System of Eye
Practice Questions
Visual Acuity and Contrast Sensitivity
Practice Questions
Refractive Errors
Practice Questions
Accommodation and Presbyopia
Practice Questions
Optical Instruments
Practice Questions
Lenses and Prisms
Practice Questions
Retinoscopy
Practice Questions
Subjective Refraction
Practice Questions
Contact Lens Optics
Practice Questions
Wavefront Technology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app